Now that conductive keratoplasty with the Viewpoint system from Refractec has been approved for over a year, and some patients are at their four-year follow-up points, surgeons are getting a clearer picture of what the procedure's limits are. Some users say that, due to regression, it may be most effective for hyperopia of around 1.5 D. Surgeons who already own the devices, though, are dabbling in off-label uses that they say may be CK's even stronger suit.
CK and the Hyperope
Peter Hersh, MD, of Teaneck, N.J., and Fernando Trindade, MD, of Belo Horizonte, Brazil are two surgeons with CK patients with more than two years of follow-up. Dr. Trindade has 18 eyes from nine patients, and Dr. Hersh, who took part in CK's U.S. Food and Drug Administration study, has 80 eyes.
Dr. Trindade says that "patient satisfaction was quite high," after following the patients for almost two and a half years. He adds, however, "There is regression in every case. I think it's impossible not to have it." He says the regression is most pronounced in patients who were more than 1.5 D hyperopic before surgery. "In the +2 D to +2.5 D cases, these patients ended up +1 D or +1.75 D," he says. For all the patients, he used the nomogram provided by Refractec, and didn't overcorrect.
Dr. Hersh "essentially agrees" that +1.5 D is the level at which CK does best. "In clinical practice, we're probably not going for the 3-D maximum," he says. He adds, however, that, "I don't think we know exactly what the stability is, but, from a patient's point of view, I'm getting reasonably good clinical stability over time." Out of the 80 eyes he's treated, he's had to enhance four.
West Hills, Calif., surgeon Jonathan Davidorf has also performed CK, and gotten a sense of the possibility of regression. "Patients tend to become more farsighted with age," he says, "so we can anticipate some amount of hyperopic drift, but that's the history of hyperopia."
 |
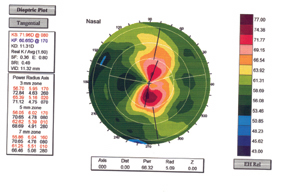 |
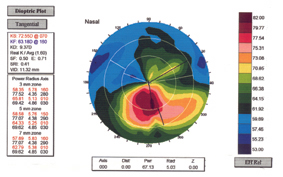
| CK for keratoconus (preop, left) can decrease the K reading and flatten the central cornea (right). | |
"The optimum treatment range is under +1.5 D," says Dr. Davidorf. "Just like in LASIK, if you go past 3.5 D or 4 D of hyperopia you might start thinking of implanting a lens, with CK, when you get above +1.5 D, you might start thinking of another procedure."
After seeing how much regression can occur, Dr. Trindade now works a substantial initial overcorrection into his treatments. "If I do a +2-D patient, my nomogram is overcorrected by 1.5 D," he says. "The nomograms have to be updated. We hope some effect will remain."
To accomplish the overcorrection, Dr. Trindade says his nomogram is "purely empirical." Instead of, for example, placing spots at the 7-mm optical zone, he puts the same number of spots in the 6-mm zone. He's not sure, however, if this is the answer. "We still have to wait a little longer to see the amount of regression after maybe five years to establish a new nomogram. I think the Refractec nomograms need to be constantly updated."
If you can afford to add another procedure to your practice's offerings, Drs. Hersh and Trindade say it does offer something of a marketing benefit, despite it's relatively low limit.
"I find that CK is more appealing to specific subsets of patients," says Dr. Hersh. "The older patient group is more laser-averse, and some view this as simpler than LASIK. It's more of a sociologic type of thing than economic, because it's a different patient group than you would normally be doing LASIK on."
"If someone comes in that's +1.5 D, LASIK is my first choice," says Dr. Trindade. "But, if the patient had any tear-film problems, I'd do CK. The beauty of the procedure is that it doesn't interfere with dry eyes and make them worse."
Off-label Applications
As some surgeons build experience with CK, they've begun using it for other procedures besides primary hyperopia. Surgeons note, however, that there are no controlled, long-term studies of CK's off-label uses. These procedures, especially for keratoconus and astigmatism, should be used with caution.
• Overcorrected LASIK and PRK. "I think it's quite good for hyperopia and astigmatism after LASIK," says Dr. Hersh. "You don't have to lift the flap, and there aren't the usual flap complications to worry about."
If a surgeon were to try it for this application, however, Dr. Hersh would advise him to use "caution and to be conservative." He believes that the procedure gives twice the level of correction as would be expected for the placement of the CK spots. He thinks this may be due to the fact that, after myopic LASIK, the central cornea is thinner and CK therefore has more of an effect. For example, in a 53-year-old post-LASIK patient, eight spots at the 8-mm zone got about 1.5 D of correction.
• Astigmatism management. Though not approved for it, CK can correct cylinder, some surgeons say. There are no established nomograms for this yet, however.
Since CK works by causing tissue to contract, the plan of attack for astigmatism is different from that of AK or astigmatic LASIK. The spots are placed in the flat meridian.
"Basically, we straddle the flat meridian at the 8-mm, 9-mm or 10-mm zone with two spots," says Dr. Hersh. In one rare case, Dr. Trindade corrected 4 D of against-the-rule astigmatism in a postop cataract patient. He says he was very aggressive with the treatment, overcorrecting the patient. Over two years, the overcorrection decayed, and the patient now only has 0.75 D of cylinder.
• Presbyopia. "The greatest patient population to treat with CK is the essentially emmetropic presbyope," says Dr. Davidorf. "We're offering them probably the safest of refractive procedures. It offers them an improvement in their near vision so they can read without glasses." He explains that, in these patients, the CK is done monocularly if they're truly emmetropic, but if they have hyperopia in the non-dominant eye, the surgeon will probably correct that too.
• Keratoconus. Dr. Trindade says that there's the possibility that CK may help patients with this condition avoid penetrating keratoplasty or even successfully wear hard contact lenses. When treatment spots are placed inside a 4-mm optical zone, rather than the usual 6-, 7- or 8-mm zone, there is a flattening effect, rather than a steepening one. "This may be able to decrease keratoconus," he says.
In three patients slated for penetrating keratoplasties for their keratoconus, Dr. Trindade used CK within the 4-mm zone. He says that the treatment "stretches" the central cornea, which can be seen on topography. The K-readings decreased from around 70 to 50.
"I was amazed to observe that the central cornea flattens to the point where the patients could have their hard lenses back," says Dr. Trindade. The patients began wearing their rigid gas permeable lenses a month after their CK procedures, and one of them has put off the PK indefinitely.
"Of course, we don't know what will happen with regression," he says.



