Radiosurgery is a technique that allows precise dissection with improved hemostasis. High frequency radio waves pass from a needle electrode through the patient to a receiving antenna. As the needle electrode touches the tissues of the body, the high frequency waves cause the cells to volatilize. Damage to the surrounding tissues is minimal because there is very little lateral heat generated. By varying the waveform, the surgeon can keep the bleeding to a minimum.
Many people who desire an upper lid blepharoplasty have lateral brow ptosis. A lateral brow lift usually enhances the blepharoplasty effect for people with excess upper lid skin. This procedure is less invasive and less time consuming than an endoscopic or coronal brow lift. It does not have the same versatility as the more extensive procedures but it is useful in some patients with excess lateral upper lid skin.
With the Ellman Dual Frequency Surgitron (Ellman Intl.., Hewlett, N.Y.), I can perform an upper lid blepharoplasty with minimum bleeding. Through the same incision, I dissect between the brow and the underlying periosteum. Less bleeding in this normally vascular area allows me to visualize the anatomy better and perform the brow lift more easily.
Procedure
I draw lines to outline the amount of excess skin to be removed. The patient is awake during this time because I want him to look up to indicate the upper lid crease. I manually put the brows in the desired anatomic position before I draw the lines with the patient lying down. This is done to prevent taking too much skin and finding that the patient can't close his eyes once the brows are lifted. I follow the general rule that there should be about 1 cm of skin between the lower brow hairs and the upper lid crease and about 1 cm of skin below the upper lid crease after the blepharoplasty incision has been closed. The medial end of the lines is just above the superior punctum and the lateral extent is usually 1 cm lateral to the lateral canthal angle. Once the lines are drawn, I prep the lids and inject with 2% lidocaine with epinephrine.
 |
 |
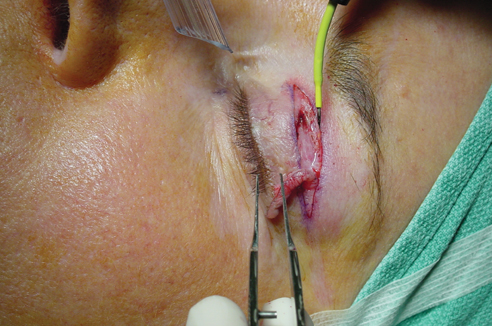
| Better visualization and decreased bleeding are two of the benefits of the radiosurgery procedure with the Ellman Dual Frequency Surgitron. |
After the skin incisions are made, the Empire Needle is used to cut a skin muscle flap. I usually use a hemo setting on a relatively high power. The thicker electrode presents a wider surface than the thin A-10 needle. Increased area of contact between the electrode and the tissue, combined with the hemo setting, will give more lateral heat and better hemostasis.
I continue using the Empire Needle to dissect between the periosteum above the superior rim and the subcutaneous tissue beneath the brow. There should be a sufficient amount of tissue beneath the skin so that the suture used to fix the brow will not cause a dimple in the skin. To keep bleeding to a minimum, I use the hemo setting. This is a vascular area and a large bleeder may be encountered. If this occurs, I use the Ellman bipolar forceps set on the bipolar mode.
I dissect about 1 cm above the superior orbital rim in a line above the lateral canthal angle. I pass the needle of a 4-0 polypropylene suture through the skin in the area of the inferior brow hairs in a line above the lateral canthal angle.
The needle exits through the muscle under the brow and is then passed through the periosteum about 1 cm above the superior orbital rim. I then pass the needle back through the muscle or subcutaneous tissue under the inferior part of the brow to meet the other end of the suture that was passed through the skin to exit through the muscle. The end of the suture without the needle is now brought through the skin. I tie the suture in a loop to fix the brow to the underlying periosteum. I am essentially attaching the underside of the brow to the periosteum about I cm above the superior orbital rim. I find that it is easier to identify the proper placement of the suture under the brow by first passing it through the skin near the brow.
 |
 |
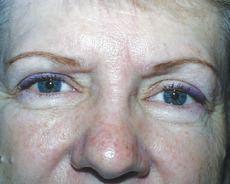 |
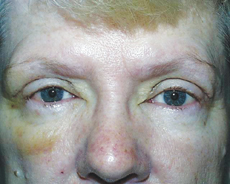
| These preoperative (top) one-week postop (middle) images show little bruising following bilateral upper lid blepharoplasties and a right brow lift using radiosurgery. Bottom, the patient at five weeks. |
I close the blepharoplasty with a running 7-0 polypropylene suture. Loops are tied at each end of the suture. This maneuver facilitates suture removal. Seven to 10 days after surgery, the loops are cut and the suture is slid out.
A browpexy enhances the effect of an upper lid blepharoplasty, especially if there is lateral brow ptosis with lateral hooding. Radiosurgery can facilitate this procedure because of the increased hemostasis available during dissection.
Dr. Older is an affiliate professor of ophthalmology at the University of South Florida College of Medicine in Tampa, Fla. Contact him at (813) 971-3846 or cecsadmn@tampabay. rr.com. He also conducts three- to five-day mini-fellowships on radiosurgical techniques in oculoplastics. Information on these is available at ellman.com. Dr. Older receives honoraria from Ellman.


