From diagnostic applications to guiding customized ablations, wavefront data have a variety of uses in clinical practice. However, while using wavefront data for customized LASIK has been successful, interpretation of individual values for diagnostic purposes remains difficult.
"As a purely diagnostic tool, physicians are learning how to look at wavefront data and interpret them to add some diagnostic value to their patient assessment," says John A. Vukich, MD, assistant clinical professor at the University of Wisconsin, Madison.
Another use for these data is to understand the symptomatology of patients who have already undergone refractive surgery. Wavefront data are being used to try to interpret post-refractive surgery patients' visual complaints, says Douglas D. Koch, MD, professor and the Allen, Mosbacher, and Law Chair in Ophthalmology at Baylor College of Medicine's Cullen Eye Institute, Houston. "Having said that, we still lack a satisfactory way of interpreting patients' wavefront data because we know that different wavefront aberrations interact in different ways," he adds. "Two aberrations that might independently lead to some noticeable visual loss might not lead to significant loss when combined. We don't have the kind of one-to-one correlation between either total higher-order aberrations or any one given aberration and patient symptoms."
Wavefront Measurement
According to Stephen D. Klyce, PhD, wavefront measurement devices use one of four different technologies, and all four technologies are capable of producing the same data.
 |
The most commonly used technology is Shack-Hartmann, which uses an array of lenslets to image different parts of the pupil. The second technology is ray tracing, which is used by Tracey Technologies, LLC (Houston). "This device uses a laser beam projected at the retina and observes the position of that beam as it comes back. It projects these laser rays sequentially so that there is no confusion about the location of the entry point and the location of the exit point, which can be a problem in very aberrated eyes using the Shack-Hartmann technology," says Dr. Klyce, professor of ophthalmology and anatomy/cell biology at Louisiana State University and adjunct professor of biomedical engineering at Tulane University.
Dr. Klyce noted that, with Shack-Hartmann, all of the rays are looked at simultaneously. If there is enough distortion in the eye, there can be some overlap and confusion. While ray tracing technology has this advantage over Shack-Hartmann, it also has limitations. Dr. Klyce says that because these projections are done sequentially, the measurement can take a significant amount of time and the data can become confused by eye movements.
The third technique being used is a modification of skiascopy (retinoscopy). The Nidek OPD Scan (Fremont, Calif.) employs dynamic skiascopy. Using a series of sensors that rotate very rapidly, the device can collect more than 1,400 retinoscopic data points in a short period of time, Dr. Klyce explains.
The final technique is the Tscherning method, which projects a grid or pattern onto the retina and evaluates the distortion of that pattern as a means to measure the wavefront of the eye. "This methodology is essentially the same as ray tracing technology," Dr. Klyce says.
Customized Laser Ablations
Surgeons agree that wavefront data are most valuable for guiding customized laser ablations. Marc Mullie, MD, believes that all refractive surgery patients should receive wavefront treatment, because customized LASIK induces fewer higher-order aberrations than conventional LASIK. "No matter what refractive surgery you do, you will usually induce some higher-order aberrations, but we're great believers that all patients should have customized treatments because if there is less chance of inducing aberrations, then the result is likely to be better," says Dr. Mullie, who is in private practice in Montreal.
Refractive Surgery Enhancement
Dr. Mullie also uses wavefront data for refractive surgery retreatments or custom upgrades. This is an off-label use of the technology in the United States.
He believes that analyzing wavefront data is especially useful for retreatments. "If a patient who has had previous refractive surgery complains of specific symptoms such as ghosting or excessive halos or glare at night and you can match wavefront measurements to his or her symptoms, then this patient is probably a very good candidate for enhancement with wavefront surgery," he says.
Daniel S. Durrie, MD, notes that getting good data is especially important in these patients, because these cases are often more complicated than primary procedures. "All of the instructions for the laser come from the wavefront device, so delegating measurement to a technician and not looking at it closely is equivalent to turning over all of your refraction and surgical planning to a technician," says Dr. Durrie, director of Durrie Vision PA, and an associate clinical professor at University of Kansas Medical Center, Kansas City, Kan.
He believes that delegating this important step often results in the "garbage in, garbage out phenomenon." Dr. Durrie says that a number of things can influence data, such as tear film or eyelashes being in the way, the pupil not being dilated enough, dry eye, or the patient being caught during a blink.
In addition, corneal incisions can be misinterpreted by the machine as distortions, and patients' focusing needs to be controlled, he adds. "Visx (Santa Clara, Calif.) suggests that patients not be dilated, which means they can still focus," says Dr. Durrie. "So, your technician needs to make sure that the patient is not focusing on the wrong target. If this happens, you will get bad data because the patient's focusing ability is misinterpreted as being nearsightedness. If you just pay attention, all these things can be avoided."
Dr. Durrie says that even if technicians are experienced at performing wavefront measurements on virgin eyes, surgeons should look over technicians' shoulders on eyes that have already undergone refractive surgery.
Diagnostic Uses
While wavefront data have the potential to be used for diagnostic purposes, there is still a lot of work to be done so that the information can be presented to physicians in a useful way.
Dr. Vukich says that wavefront information alone without considering the rest of the clinical picture has limited value. "It has proven very difficult to look at a single metric, whether it is RMS [root mean square] value or an individual Zernike component, and predict what quality of vision a patient may have or predict what is causing the aberration in the first place," he says.
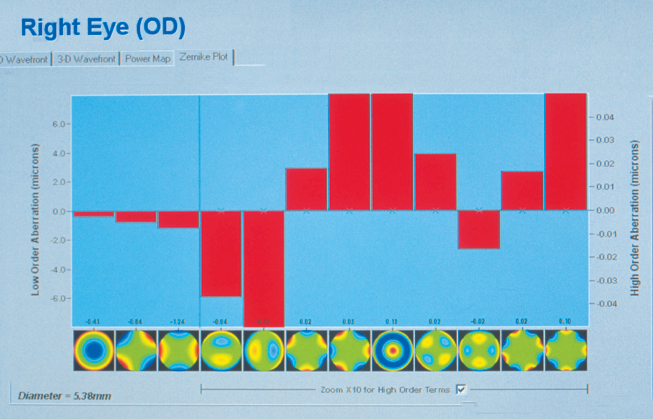 |
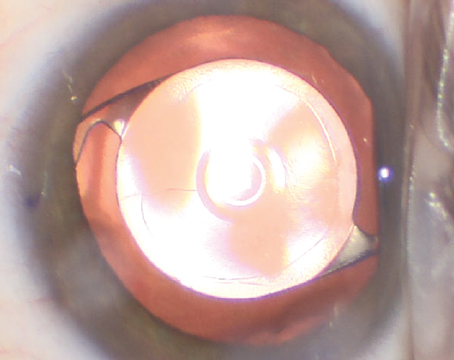
| Alcon's current LADARWave software provides a graphic depiction of specific higher- and lower-order aberrations in each eye. |
In certain patients, however, wavefront information can be useful to confirm a diagnosis. Dr. Koch recently used wavefront data to diagnose a young man who presented in his office complaining of worse vision in bright light and sunlight. "This is somewhat atypical," he says. "Wavefront aberration data showed that he had a tremendous amount of spherical aberration, and we found that he has anterior lenticonus. It was very subtle visually to detect it at the slit lamp, but it was really brought out by the wavefront."
Zernike polynomials provide a mathematical description of the optical aberrations, but interpretation of these individual values remains difficult. "The Zernike polynomials are able to extract higher-order terms than the spherocylindrical terms, and some of these are useful to know," Dr. Klyce says.
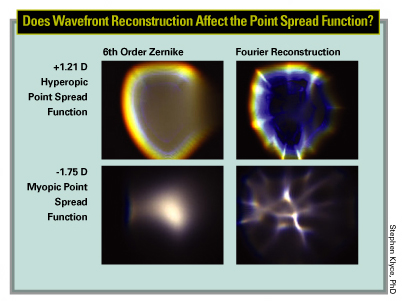
He explains that wavefront is measured at the pupil plane. If that same information is projected to the back of the retina, it forms a point spread function. If the point spread function looks like a comet, the patient has coma, he says.
"Diagnosticians are learning to use these pieces of information to try to figure out what is wrong with the optics of the eye. However, there have not been published standards that display wavefront information that have been accepted on a broad scale," he says.
Dr. Klyce notes that corneal topography is still important and that a combination of information from wavefront and corneal topography is the future of how the best systems will correct aberrations of the eye.
One problem with using wavefront data for diagnostic purposes is that most wavefront machines present information in microns, while most clinicians think in terms of diopters of power or curvature change, Dr. Klyce says.
Some instruments, such as the Nidek OPD Scan, present data in diopters. One can compare the wavefront data presented in diopters directly with corneal topography presented in diopters. This allows clinicians to immediately see if the wavefront errors within the pupil are emanating from similar aberrations on the corneal surface or whether they are coming from inside the eye.
Dr. Klyce says that Nidek has developed a display called the internal aberrations map, which is the difference between the total aberrations of the eye measured with the OPD map and the refractive power of the corneal surface. "This is a very useful clinical tool that is just now coming into its own and is currently being tested," he says.
Dr. Vukich says that physicians are still trying to figure out what to do with wavefront data as far as making a diagnosis. "The data are there, and clearly there is a lot of information. There has been a lot of work done with point spread functions, and that seems to hold the most promise for a descriptor of the visual system that approximates more closely what the patient actually sees," he says. Point spread functions seem to have a very good correlation with patients' visual phenomena, according to Dr. Vukich.
Zernike vs. Fourier Analysis
While all wavefront devices currently use Zernike polynomials, wavefront device manufacturers are considering other algorithms. Stephen G. Slade, MD, says Visx has recently resurrected Fourier analysis and is looking at the advisability of employing it to measure aberrations and then using it to express the changes to the laser.
"Visx believes that it can get a finer gradation of assessment with Fourier analysis," says Dr. Slade, assistant clinical professor, University of Texas, Houston. "Fourier analysis may be a more practical way to express information, because as you are getting finer in the gradations, the mathematical formulas become more complex, and the computing power needed to process them must increase."
However, while Visx believes Fourier analysis will produce better results, Dr. Slade says that the other laser companies have countered that the higher levels of aberration that Fourier analysis will detect cannot be treated.
Dr. Slade says that this is currently an unresolvable issue. Clinical studies are needed to determine whether Fourier analysis is better than Zernike polynomials in measuring wavefront data.
Additionally, he says that wavefront results are so good that companies may be reaching the area of diminishing returns: Improvements may not offer any practical benefit. "Of more interest to me is how to treat highly aberrated eyes or how to treat when there is not enough tissue or an unstable cornea," Dr. Slade says.
Dr. Durrie says that all laser companies should be looking at improving treatment. "If we have preop wavefront measurements and postop wavefront measurements, the companies can look at both data sets to determine where to put more pulses. Always striving to get better clinical results should be the goal for all the companies," he says.
Dr. Koch says that Visx is also developing a chromatic point spread function (i.e., one that takes into account chromatic aberrations). "This is how our patients see," he says.
He noted that patients don't just see one wavelength of light, which is how all current wavefront analyses are performed. Dr. Koch says studies have shown that Zernike polynomials miss data in patients with higher amounts of irregular astigmatism. "The point spread function generated by Zernike polynomials isn't as representative of what the patient actually sees," he says. "We often are unable to correlate the point spread function that shows up on the machine with a patient's own symptoms. I think Fourier analysis will give a more accurate representation of the actual optics of the eye, and combining this with a chromatic point spread function should in theory provide the best available representation of patients' vision."
Dr. Vukich agreed, noting that a polychromatic point spread function goes even further to refine the expression of what the visual system is seeing at the level of the retina.
Extending the Boundaries
Dr. Durrie noted that Alcon (Fort Worth, Texas) has developed a new algorithm called the extended range algorithm, and Dr. Mullie says that all of the laser companies are working to get better registration. Dr. Mullie says that Bausch & Lomb (Rochester, N.Y.) is working on a new system for registration called Iris Recognition Software. Because each person has a unique iris, iris recognition is already being used in some security systems. "The same thing can be done with wavefront," he says. "You can take a picture of the iris when you take the wavefront measurement. Then, when the patient lies down for treatment, the computer can match the preop iris details to the current details. The computer can then rotate the wavefront treatment into the correct position."
Dr. Klyce noted that Nidek, Visx and other laser companies have systems in place for cyclotorsional registration using iris features. Additionally, the LADARVision System was the first laser system to employ eye tracking using NASA technology, he says.
While the Bausch & Lomb Iris Recognition Software is currently available in other countries, it won't be available in the United States until sometime in 2005, says Dr. Mullie.