In ophthalmology there are very few, true "emergencies." Pathology such as ruptured globes or acute angle-closure glaucoma are considered emergencies because they are vision-threatening and need to be managed in a timely fashion. However, orbital compartment syndrome is a true ocular emergency; rapid diagnoses and treatment are essential to prevent permanent vision loss.
OCS is defined as elevation of intraorbital pressure that results in impaired vascular perfusion of the optic nerve and globe. The most common cause is post-traumatic retrobulbar hemorrhage. However any process that increases intraorbital pressure acutely can cause a compartment syndrome. Therefore acute inflammation or infection, emphysema or air in the orbit after a patient with an orbital fracture blows his nose, or rapid growth of a neoplasm can cause OCS. Certainly OCS can also be caused iatrogenically; one of the most feared complications of eyelid and periocular surgery is a retrobulbar hemorrhage. Less commonly recognized iatrogenic causes include inappropriate use of packing during orbital or sinus surgery, thrombolysis for myocardial infarctions or stroke, and inadvertent "leaning" on an eye during periocular surgery can cause increased orbital pressure leading to OCS.
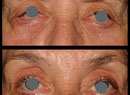
In the typical case of OCS, patients present with acute onset of pain and proptosis. In the case of a retrobulbar hemorrhage, tense eyelids with ecchymosis defined by the orbital rim are classic. If the eyelids are forced open, motility is markedly decreased and vision is variably decreased as well (See Figure 1). As with any acute compressive optic neuropathy, an afferent papillary defect may be present. Intraocular pressure is highly elevated, and funduscopic examination may reveal retinal venous congestions, central retinal artery pulsations, retinal edema and optic disc swelling.
The key to managing OCS is making the clinical diagnosis and treating with soft tissue decompression of the orbit. The mistake clinicians may make is to suspect OCS but rely on secondary imaging studies to confirm the diagnosis. Untreated, irreversible damage can take place in as short as 90 minutes of ocular ischemia time. So waiting for a diagnostic study is not advisable. Likewise, if you are consulted over the phone for a suspected OCS and patient transit would take longer than a few minutes, you might consider finding someone local who can treat the OCS rapidly, in the extreme case you may need to teach someone over the phone how to address OCS.
OCS occurs because the orbital septum is tightly adherent to the orbital rim at the arcus marginalis, creating the orbital compartment. Therefore, bleeding or a space-occupying process will cause OCS. To release this compartment, lysis of the lateral canthus and inferior crus of the lateral canthal tendon is very effective. Although authors have described direct draining of hematoma or bone-decompression for OCS, it is not necessary.
To release the lateral canthus, an incision between the upper and lower eyelids through the lateral commissure is performed with scissors after instillation of local anesthetic (See Figure 2). Then the inferior crus of the lateral canthal tendon is 'strummed' by the scissors and lysed (See Figure 3). Successful release of the lateral canthal tendon and inferior crus will allow the eyelid to easily evert and the globe to sublux forward. This subluxation is beneficial, and the optic nerve will not be compromised by the anterior displacement of the globe. Decrease in intraocular pressure should result after release.
Post-surgical management can include imaging studies and prophylactic antibiotics.
Repair of the lateral canthus should be delayed up to a week, although oftentimes the wound will heal without intervention.
Dr. Bernardino is at the Yale University School of Medicine, Department of Ophthalmology, Section of Ophthalmic Plastics and Orbital Surgery. Contact him (203) 785-2020 or robert.bernardino@yale.edu.