BFTA vs. BFS
Bordeaux, France, ophthalmologist David Smadja and his research co-workers say that when they focused on the asymmetry of the cornea’s posterior surface, they were able to achieve excellent sensitivity when screening patients for keratoconus.
Dr. Smadja, who used the Ziemer Galilei dual Scheimpflug system, says the key is studying a parameter known as the Best-fit Toric and Aspheric surface, or BFTA, which seems to be a better option than the Best-fit Sphere, or BFS. “The BFTA has a better ability for screening out the asymmetry of the cornea that is measured because it fits closer to the natural corneal shape by canceling out its means asphericity and toricity,” explains Dr. Smadja. “What is nice about the BFTA is that comparing a cornea to it is almost like comparing the cornea to its perfect clone. Therefore, anything that will deviate from the reference surface will be a sign of irregularity or asymmetry. This method is important because when you’re tracking the initial signs of asymmetry, if you don’t want to have the initial bulging hidden by the effect of another fitting method—such as with the spherical reference surface, the BFS—it’s important to be as close as possible to the cornea being measured.
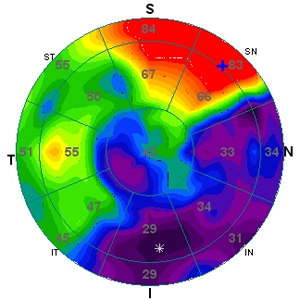
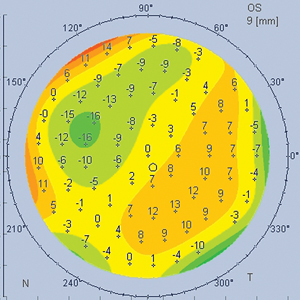
“Comparing it to the BFS, it’s not a matter of one being better or one being bad,” Dr. Smadja continues. “Some people are used to seeing and interpreting BFS analyses and sometimes it’s a matter of subjective interpretation of elevation patterns. So if you’re used to using the BFS, it can help screen out suspect corneas—but more often with the BFS, the elevation maps can hide crucial early signs of asymmetry in the cornea. In our study, when we compared the BFTA to the BFS to screen out the initial stage of keratoconus, we found the performance of the BFTA to be much higher than the performance of the BFS in terms of discriminating between normal and forme fruste keratoconus.1 Specifically, when looking at the maximum posterior elevation, BFTA yielded a sensitivity of 82 percent and a specificity of 80 percent, compared to 51 percent and 55 percent, respectively, for the BFS. This sensitivity of 82 percent with the BFTA was then improved to nearly 90 percent when looking at the AAI [Asphericity Asymmetry Index], which quantifies the asymmetry of elevation at the back surface by using the absolute value of the max positive and max negative elevation within the 6-mm central zone. The AAI has a cutoff value of 21.5.”
|
For surgeons who want to use some of Dr. Smadja’s findings in their practices, he has some advice. “It’s tough to give a number that would be a red flag with all the various devices, because we haven’t tested this approach with all of them,” he says. “However, what should alert the surgeon when interpreting posterior elevation maps with either the Aconic surface (Orbscan) or the Best-fit Toric Ellipsoid (BFTE) in the Pentacam, which work in a way similar to the BFTA in the Galilei, is any kind of asymmetric posterior elevation. Concerning the Galilei Analyzer specifically, the AAI was found to be the most sensitive for screening the suspicious cornea. Any AAI value above 21.5 should make you consider doing PRK rather than LASIK.”
Epithelial Analysis
Focusing on a different parameter of the cornea, researchers in Greece have found that using anterior segment optical coherence tomography to image the epithelium showed marked differences between keratoconic and normal eyes.
In a study presented at the 2013 meeting of the American Academy of Ophthalmology, George Chatzilaou, MD, presented results from 55 untreated keratoconus patients and 55 controls. The mean overall epithelial thickness was 55.65 ±1.22 µm in the keratoconus patients and 51.97 ±0.7 µm in the controls. The variability in topographic mapping was ±9.8 ±0.41 µm in keratoconus eyes and ±1.53 ±0.21 µm in normals. All the differences were statistically significant (p<0.002). The researchers say that these patients seemed to have an overall epithelial thickness increase.
Athens surgeon John Kanellopoulos was a researcher on the study and says it yielded some insights on irregular corneas. “We all know that in keratoconus the cornea epithelium remodels and it thins over the area of the cone and thickens over the area adjacent to the cone in order to ‘mask’ these curvature differences and potentially improve the visual function of the cornea,” he says. “So the first thing that we look at in these spectral domain anterior segment OCT images is: Where is the thinnest location placed by the device in regard to the cornea center? When the thinnest part of the cornea is away from the cornea center, our index of suspicion for keratoconus increases, as this indicates an eccentric thinner part of the cornea, which invariably is due to keratoconus or ectasia.
“Now, what we have reported in the past with high-frequency ultrasound,” Dr. Kanellopoulos adds, “and we confirmed with our studies with a spectral domain anterior segment OCT, is that is there a very large difference in different areas and in different aspects of the cornea as far as the thickness—so increased variability of the cornea epithelial thickness can be related to keratoconus. In addition, we’ve found that, overall, the epithelial thickness is increased in keratoconic or pre-keratoconic eyes, as well. So just looking at the average corneal epithelial thickness can be a very helpful tool in picking up early keratoconus, because advanced keratoconus is obviously much easier to diagnose from the extreme irregularities of the epithelial distribution in the cornea.”
Whichever method a surgeon uses, Dr. Smadja notes that more information is always better. “It’s important to remember that in our work, we’re still just talking about one parameter,” he says. “The sensitivity achieved by one parameter is never good enough to base your conclusion on. I think that it’s best to consider different parameters when considering a change to the patient’s surgical options.” REVIEW
1. Smadja D, Santhiago MR, Mello GR, et al. Influence of the reference surface shape for discriminating between normal corneas, subclinical keratoconus, and keratoconus. J Refract Surg 2013;29:4:274-281.