Angle-closure glaucoma is a major problem around the world. Although its prevalence varies from one ethnic group to another—it's very common among those of Chinese or Indian descent, less so among African Americans and Caucasians—overall it's more widespread than open-angle glaucoma. And of all glaucomas, it causes the greatest amount of blindness.
The problem in most angle-closure glaucomas is typically that the iris has been pushed upward by a pupil block mechanism and/or the crystalline lens, and it's obstructing the meshwork in the area of the angle and preventing aqueous from reaching the outflow channels, leading to increased intraocular pressure. When the iris is first pushed upward, the iris and the peripheral cornea are simply appositional; over time, however, synechiae can develop between them.
Unfortunately, this condition is probably underdiagnosed. Gonioscopy is often not performed, and when it is, it's prone to artifact. The surgeon tends to push on the eye while using the gonioscopy lens, and shining a light into the eye to improve visibility constricts the pupil and opens up the angle artificially, leading to a potential misdiagnosis. Many times, patients have been referred to me with "open-angle glaucoma"; upon closer examination I find that the mechanism is actually angle closure. (To avoid this kind of misdiagnosis, we use anterior segment optical coherence tomography to visualize the angle. Because OCT uses infrared light, the pupil doesn't constrict and we get a more natural view of the angle.)
Traditional Treatment Options
When a surgeon does diagnose closed-angle glaucoma, the first-line treatment is typically laser peripheral iridotomy, with or without laser peripheral iridoplasty; this can work well in cases were the iris is predominantly appositionally closing the angle. In cases of uncontrolled IOP despite laser/ medical therapy, the traditional response has been either to go straight to trabeculectomy or to address the problem with a goniosynechialysis by trying to move the iris away from the angle with a blunt-tipped cyclodialysis spatula or a knife.
Both approaches have drawbacks. Trabeculectomy doesn't address the cause of the problem—the blockage of the trabecular meshwork—and it creates a bleb, accompanied by the usual risks and potential complications. The second option involves inserting a cyclodialysis spatula into the eye through the anterior chamber, engaging the periphery of the iris and then pushing down on the iris to separate the tissues and release the synechiae. Unfortunately, this isn't very ergonomic; often the synechiae are dense and difficult to release, and if you use too much pressure, you can cause bleeding. 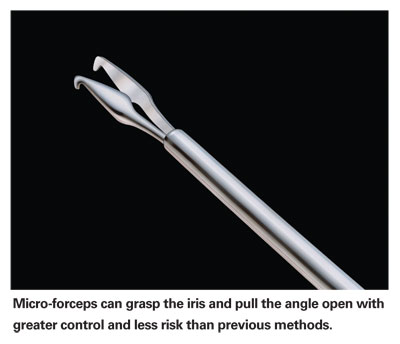
Some surgeons have also done this using a goniotomy blade. The problem with this approach is that a goniotomy blade is a sharp instrument; a misstep could result in cutting out to the angle and damaging the meshwork. In fact, you don't need to cut the iris loose—it separates from the opposing tissue when pressure is applied. It's stuck by apposition, not because it has grown into the angle.
The other issue in goniosynechialysis is intraoperative visualization. Some surgeons using these approaches don't attempt to view the procedure while performing it; they simply examine the angle beforehand and afterwards. This adds to the uncertainty of the result and potential for excessive force and resulting bleeding. A goniotomy lens (i.e., Swan Jacob lens) can be used, but this requires rotation of the patient's head and eye position. Alternatively, an indirect gonioscopy lens may be used.
Using Micro-Forceps
Recently, I developed an alternative method for separating these tissues that offers several advantages over the traditional alternatives. This approach, in which the surgeon grasps the iris with micro-forceps and gently pulls it free with a central vector motion, occurred to me because I recently helped to create a tool of this type. The forceps I designed, called a "micrograsper," is part of a set of micro-tools intended to make it easier for cataract surgeons to manipulate tissues in the anterior chamber. This particular instrument is useful when managing dislocated intraocular lenses or suturing inside the eye, as well as for holding the iris during repair or reconstruction. It occurred to me that it might also provide an excellent way to perform synechialysis.
To perform synechialysis using the micro-forceps, the tool is inserted through a small incision; the small size of the incision helps to maintain the anterior chamber. (A cohesive viscoelastic such as Healon 5 can be injected into the chamber as well.) Instead of applying downward pressure to separate the tissues, as you might with a spatula, I grasp the iris and gently pull it away from the angle toward the center of the pupil. The vector force is completely different, and the process is far easier to control; the forceps allow you to apply just the right amount of pressure.
The second key factor that makes this process ergonomic is using an indirect goniotomy mirror to view the angle as the tissues separate. As the angle opens the angle structures become visible, so I can tell when I've reached my endpoint. Of course, dynamic viewing is also possible when using a spatula or knife to separate the tissues, but the motions and force vectors make it more difficult to evaluate what's happening.
Manipulating the tissue and viewing the procedure through a gonio lens in real time does require a little orientation to maximize your hand-eye coordination, especially since the mirror inverts the image. However, it's not that big a learning curve, and the advantages are well worth the effort.
In the OR
The entire process of goniosynechialysis only takes about five minutes. I work with 20 to 30 degrees of the iris at a time, and it releases very easily. The only area that's a little difficult to manipulate is the tissue right below the incision you make. You can manage this by simply grabbing the iris a little farther away from the area you're releasing, or by working through another incision 90 degree away. Since we usually combine this procedure with cataract surgery, we can easily use the sideport incision to approach from a different angle.
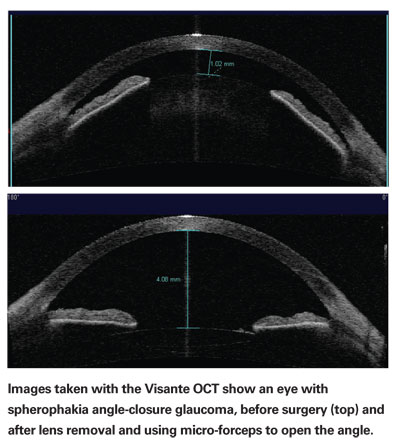
The reason for combining this with cataract surgery is that removing the lens helps to deepen the angle. Generally, part of the pathogenesis of angle-closure glaucoma is that the lens takes up a large amount of space within these eyes, predisposing shallowing of the anterior chamber and angle closure. By removing the lens, you're typically replacing a 4- to 5-mm thick lens with a 1-mm thick implant, which helps to prevent a recurrence.
Another helpful strategy, especially when you're first attempting this, is to inject a little acetylcholine (Miochol-E or Miostat, Novartis Ophthalmics). This causes the pupil to constrict, drawing the iris away from the angle. Next, inject a bit of viscoelastic. At this point the chamber is deepened, the eye is stable and the iris is away from the cornea. This also helps to ensure that there's no chance of accidentally grabbing the capsule or touching the IOL when you're just getting used to performing the procedure.
One of the advantages of this procedure is that it has few risks and complications. Occasionally, these patients retain a little viscoelastic, and they can have some inflammation. It's also possible to initially see an IOP spike that may last a few days as the meshwork regains function. To prevent this from being an issue, I recommend increasing glaucoma medication during this period, including Diamox, and putting these patients on intense anti-inflammatories for the first few days. Probably the biggest issue in terms of complications is bleeding. However, this is very uncommon—certainly less common than when using a spatula, which gives the surgeon less control.
Excellent Results
At this year's meeting of the American Glaucoma Society we presented results of a study we conducted, using this technique on 34 patients whose angle closure resulted from spherophakia, in which the zonules are abnormal—typically from birth—leading to a rounded lens that can move forward and precipitate angle closure glaucoma. After lens replacement and goniosynechialysis using this technique, average best-corrected acuity went from 20/60 to 20/30; mean IOP dropped from 26.3 mmHg to 14.8 mmHg; and the number of meds required to maintain IOP dropped from 3.2 to 0.7. More than 91 percent of the patients achieved pressures below 21 mmHg without further surgery. There were no intraoperative complications; postop, 10 patients (29.4 percent) experienced an IOP spike; six developed uveitis that resolved; and four had transient hyphema. Two of the 34 eyes with advanced disc damage later required trabeculectomies.
In a similar, smaller study involving 15 primary angle-closure glaucoma patients, visual acuity improved from 20/100 to 20/40; mean IOP dropped from 38 mmHg to 16.4 mmHg; and number of meds required dropped from 3.8 to 1.3. In this study, there were no intraoperative or postoperative complications.
In terms of maintaining these results long-term, our data now include patients who have been stable for several years. Also, published literature regarding the use of some of the other techniques that achieve the same result has shown that the benefits last for at least a number of years.
Getting Started
If you're interested in trying this procedure, you should begin by familiarizing yourself with the skills involved. It helps to be comfortable and proficient with gonioscopy; you definitely should not attempt this if you have no experience with a gonio lens.
To increase your proficiency, I'd begin using an intraoperative gonio lens, even on routine cataract cases, to visualize the angle during and after the case. Then, I would start placing a pair of the forceps through an existing incision to get comfortable with manipulating them inside the eye, while viewing with the mirror. The object would not be to grab any tissue, but simply to get a feel for manipulating with the forceps while observing through the lens. Then, when a suitable case turns up, you'll be able to use this approach comfortably.
The ideal candidate is a patient with either acute or chronic angle closure. It's best to do the procedure early on, because over time, the tissue may grow into the opposing tissue. Also, you should initially pick patients who don't need to achieve a very low target pressure, since that might require a trabeculectomy to achieve. (If the angle is closed for other reasons, such as neovascular, iridocorneal endothelial syndrome or uveitic glaucoma—you shouldn't use this method.)
A Promising New Approach
Performing goniosynechialysis using micro-forceps is very safe, and the results have been impressive; our success rate is well above 90 percent, complications have been minimal, and the benefits appear to be long-lasting. Essentially, this method allows us to restore physiologic outflow without creating a bleb, while leaving open the possibility of trabeculectomy at a later date, should that become necessary. Given the widespread incidence of primary closed-angle glaucoma around the world, every new tool is a step in the right direction.