A 46-year-old, otherwise healthy Caucasian female presented to the Wills Eye Emergency Department with a five-day history of visual changes in the left eye, including distortions and grey scotomas in her vision. The symptoms had been stable for the past five days. She denied any concurrent headache, photopsias or ocular pain. The patient denied any recent illnesses. Systemic review of systems was unremarkable. Ocular history was significant for contact lens use and blepharitis controlled with warm compresses and preservative-free artificial tears.
Medical History
Past medical history was insignificant, and the patient was not taking any systemic medications. Family history was significant for heart disease, hypertension, diabetes and thyroid disease. The patient drank alcohol socially, but did not smoke or use illicit drugs. She was allergic to Compazine, which resulted in a dystonic reaction.
Examination
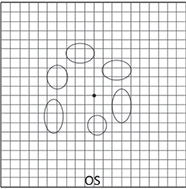
The patient’s vital signs were stable and within normal limits. Ocular examination demonstrated a best corrected visual acuity of 20/20 in both eyes. Her pupils were equal, round, reactive and without any relative afferent pupillary defect. Extraocular motility was full OU, and there was no pain elicited on ocular motility. Visual fields were full to confrontation OU. Ishihara color plates were full and brisk bilaterally. An Amsler grid was unremarkable in the right eye, but demonstrated paracentral grey scotomata in the left eye (See Figure 1).
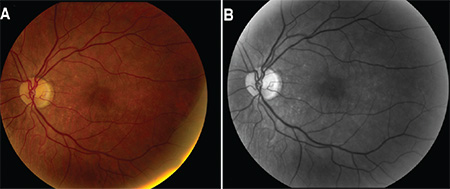
External examination was unremarkable. Anterior slit-lamp examination demonstrated blepharitis, inferior superficial punctate keratopathy and trace nuclear sclerosis OU. Intraocular pressure by Goldmann tonometry was 14 mmHg OD and 14 mmHg OS. Fundoscopic examination OD demonstrated a clear vitreous and an optic nerve with sharp margins, good color and a cup-to-disc ratio of 0.1. The vessels were normal in caliber and the macula appeared flat and without any hemorrhage, exudates or pigmentary changes. There was cobblestoning of the inferior retina peripherally. Fundoscopic examination OS (See Figure 2A) demonstrated trace vitreous cell and an optic nerve with sharp margins, good color and a cup-to-disc ratio of 0.1. The vessels were normal in caliber, but the macula demonstrated foveal granularity and scattered pigmentary changes throughout. There was cobblestoning of the inferior retina peripherally. Red-free fundus photography was performed OU (See Figure 2B), which further highlighted these pigmentary changes OS.
|
Please click this link for diagnosis, workup, treatment and discussion.


