A 2-year-old boy presented to the ophthalmologist two weeks after his mother noticed his left pupil appeared “cloudy” compared to prior photographs. The patient’s mother didn’t notice any other local changes such as trauma, infection or pain, and the child was otherwise healthy.
Medical History
The patient was a fraternal twin born at 36 weeks by caesarean section. The neonatal period was complicated by a neonatal intensive care unit admission for 23 days secondary to lung
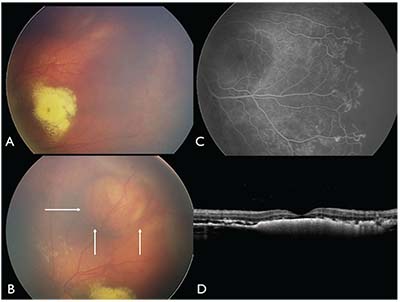 |
| Figure 1. (A) Fundus photography of the left eye on initial examination under anesthesia shows dense macular exudation and extensive subtle telangiectasia temporally. (B) A large macular cyst is seen superiorly (arrows). (C) Fluorescein angiography highlights the telangiectasia and areas of non-perfusion. (D) OCT shows dense debris under the fovea and mild cystoid macular edema. |
Examination
On ocular examination at age 2, uncorrected visual acuity was 20/40 OD by Allen testing, and it was fix and follow OS. Pupils were round and reactive bilaterally without relative afferent pupillary defect. Xanthocoria (yellow pupillary reflex) was noted in the left eye. In-office fundus examination revealed normal findings OD, and a yellow-white macular mass OS. The child was referred for an ocular oncology consultation.
Examination under anesthesia revealed prominent macular exudation in the left eye and a superiorly located retinal cyst 10 mm in diameter (Figure 1A and 1B). Subretinal and intraretinal macular exudation was confluent and intermixed with subretinal fluid, and extended to the ora serrata temporally and inferiorly. There was subtle temporal retinal telangiectasia.
Click here for Workup, Diagnosis & Discussion.


