A 62-year-old Caucasian man was referred to the Wills Eye Hospital Ocular
 |
Medical History
Ocular history included uncomplicated LASIK in both eyes 14 years prior. Medical history included cranial migraines and depression. He denied smoking and reported minimal alcohol intake. Family history was negative for cutaneous or ocular melanoma. Review of systems was unremarkable.
Examination
Visual acuity was 20/25 OU. Pupillary response, extraocular movements and confrontation visual fields were normal OU. Intraocular pressures were 10 mmHg OD and 8 mmHg OS. The anterior segment was quiet with mild nuclear sclerosis OU. There was no evidence of ocular melanocytosis.
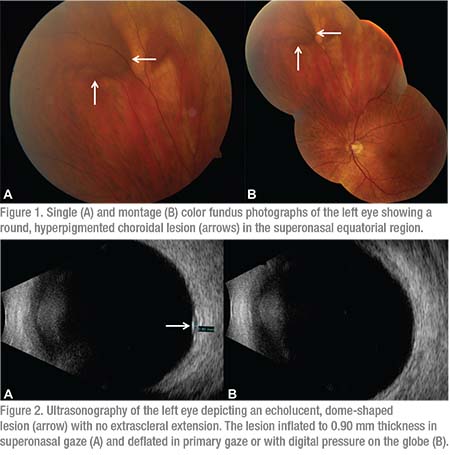
Fundus examination OD showed normal findings. Fundus examination OS revealed a clear vitreous cavity and normal macula without subretinal fluid. In the superonasal equatorial region there was a round, hyperpigmented choroidal lesion causing elevation of the retina (Figure 1, arrows). The lesion measured 6 x 5 mm in basal dimension and 0.9 mm in ultrasonographic thickness (Figure 2A). Curiously, the lesion waxed and waned with ocular movements, inflating in fixed superonasal gaze and deflating in primary gaze. There was no hemorrhage, subretinal fluid, orange pigment or related drusen.
Click here for Workup, Diagnosis and Discussion.


