|
Three variations on the concept of placing an implant inside the cornea are in different stages of the approval process. The Kamra inlay (from AcuFocus in Irvine, Calif.) uses the pinhole principle to increase depth of field; the Raindrop (from ReVision Optics in Laguna Hills, Calif.) makes the cornea multifocal by reshaping it; and the Flexivue Microlens (from Presbia in Amsterdam) creates multifocal vision using an in-cornea lens.
Here, four surgeons with extensive experience with these options discuss what they’ve learned about them and how they may benefit your patients.
The AcuFocus Kamra
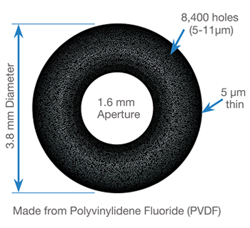
The corneal inlay closest to Food and Drug Administration approval is AcuFocus’s Kamra. “The Kamra inlay is commercially available in 49 countries, and nearly 20,000 inlays have been implanted worldwide to date,” says Minoru Tomita, MD, PhD, executive medical director of the Shinagawa LASIK Center in Tokyo, Japan, where approximately 15,000 of those cases were performed. “The inlay is 5 µm thick; it has a 3.8-mm outer diameter and 1.6-mm central aperture. It’s made of polyvinylidene fluoride and nanoparticles of carbon, with 8,400 micro-perforations that vary in size from 5 to 11 µm. The principle of the inlay’s function is similar to that of the small-aperture effect in an f-stop camera; it has minimal effect on distance image quality but improves intermediate and near image quality.”
|
Like the other inlays, the Kamra is implanted in the nondominant eye only. “The manifest refractive spherical equivalent of the implanted eye should be between -1 and 0 D right before the surgery in order to maximize the function of the Kamra inlay,” explains Dr. Tomita. “If both eyes are ametropic and presbyopic, normal LASIK is performed first to target emmetropia by making a 100-µm flap (sub-Bowman’s keratomileusis). A month later, a corneal pocket is created in the nondominant eye at a depth of 200 µm using a femtosecond laser; the inlay is inserted into the pocket.”
In terms of contraindications, Dr. Tomita says patients are excluded if they’ve had previous ocular surgeries or if they have any ocular pathology, including keratectasia, corneal degeneration, severe blepharitis, retinal disease, glaucoma, cataract, marked topographic irregularities or severe dry eyes. “If a patient with severe dry eye wants to have the inlay, we recommend that the condition be treated aggressively before the surgery,” he says.
“It’s also important to provide sufficient informed consent to the patient,” he adds. “Preoperatively, risks and precautions should be carefully explained, especially to those who are professional drivers or drive at night. Neuroadaptation is required to adjust to binocular vision with the inlay, and this takes longer as one ages. Some patients claimed they were hesitant to drive a car for up to six months after the surgery, although these conditions eventually alleviate over time.” 8,9
Dr. Tomita notes that being able to remove the inlay if the patient is unhappy is a big advantage. “Previous papers have reported that patients’ refractive state returned to within ±1 D of the preoperative refractive state after inlay removal, with no loss of corrected distance visual acuity,”10 he says. “There were also reports of good recovery of corneal topography and corneal aberrometry.11 Once the inlay has been removed, the patient can be offered other treatment options.
“The Kamra inlay is at the final stages of FDA approval,” he adds. “We hope it will be approved by the end of 2014.”
The Presbia Flexivue Microlens
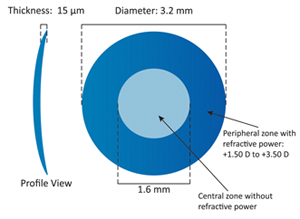
The Flexivue is a small, hydrophilic acrylic refractive inlay, 3.2 mm wide, with a 1.6-mm hole in the center. The refractive power of the ring ranges from +1.5 D to +3.5 D. Presbia announced in November that the FDA had given conditional approval to begin a Phase II trial of the inlay.
Robert K. Maloney, MD, is a clinical professor of ophthalmology at UCLA-David Geffen School of Medicine and director of the Maloney Vision Institute in Los Angeles. He is the co-medical monitor for the FDA trial of the Presbia Flexivue inlay; he has also been an investigator for the AcuFocus Kamra inlay. “The Flexivue is a crystal clear refractive inlay,” he says. “It has an index of refraction different from the cornea. There’s a small hole in the center of the inlay that provides distance vision and allows corneal nutrients to circulate freely from posterior to anterior. The inlay is designed to sit in the central cornea and create a multifocal effect so the patient gets good close and distance vision.”
Data from outside the United States has supported the effectiveness of the Flexivue. For example, in a study conducted by Ioannis Pallikaris, MD, PhD, and colleagues, presented at the 2013 European Society of Cataract and Refractive Surgery Annual Congress in Amsterdam, 77 presbyopic patients in Italy and Greece ranging in age from 45 to 60 received the implant. Average monocular UNVC improved from 20/100 preoperatively to 20/25 at one year postop, while binocular UDVA was unchanged. “The European data suggests that the inlay is very safe, and patients have been very happy,” notes Dr. Maloney.
“The inlay is typically implanted in the nondominant eye of a patient who is emmetropic in both eyes,” he continues. “It creates a slight myopic shift and a mild multifocal effect in the implanted eye, thus creating a small amount of monovision. It’s not an extreme multifocal, which could cause significant glare at night, and it’s not a full monovision, which could cause binocular disparity. So it seems to fit in a sweet spot, with a mixture of a little monovision and multifocality. That makes it very well-tolerated.”
Gustavo E. Tamayo, MD, director of the Bogota Laser Refractive Institute in Bogota, Colombia says he has implanted the Flexivue inlay in 75 patients. “I use it only in pure emmetropes, defined as those with ±1 D of sphere and ±0.75 D of cylinder,” he says. “It’s mostly being implanted in Europe, where it has the CE Mark, and South America, but it’s still not widely used; maybe 1,000 have been implanted in total.”
|
“Regarding the reduction of incoming light caused by the Kamra, one of the interesting things for me has been that patients are not complaining that their vision is dark at night,” he adds. “There may be a couple of reasons for that. First, we only implant in one eye, so the other eye is normal. Second, the Kamra inlay is about 3.8 mm in diameter, so when the pupil dilates at night light enters the eye around the outer edge of the inlay. It may be that those two factors together keep people from experiencing dim vision at night.”
Dr. Tamayo says the main advantage the Flexivue has compared to the other inlays is its more physiologic approach to correcting near vision. “Unlike the pinhole mechanism of action used by the Kamra inlay, it provides an optical correction depending on the refractive defect present,” he says. “The other advantage is the fact that it does not have any issues regarding the distribution of nutrients, which can be a factor with the Raindrop and Kamra inlays. Also, the learning curve is very small; performing the surgery is simple, fast and easy. Certainly one or two days of training would be sufficient.”
Flexivue in Practice
Dr. Maloney says the Flexivue could in theory be combined with LASIK. “You’d make a flap, correct the refractive error, place the inlay and then replace the LASIK flap,” he says. “Or it could be used with a SMILE-type procedure, in which you’d remove a lenticule through a stromal tunnel to correct the refractive error and then insert this inlay through the same stromal tunnel. But I don’t know if that’s been tried yet. Right now we’re implanting it in people who are close to emmetropia. We’re not doing simultaneous correction of refractive errors.
“In the trials, we’re using a pocket, not a flap,” he continues. “In a normal emmetrope we make a pocket with a femtosecond laser, a channel from the central cornea to the peripheral cornea with an opening in the periphery. The surgeon grasps the inlay with a special forceps and gently slides it into the pocket, centers it over the corneal light reflex and releases it, the same way the Kamra inlay is inserted.”
As far as contraindications, Dr. Tamayo says those would include the patient being unable to correct to 20/20 at near, whatever the reason. “Dry eye is not affected by the inlay, so it’s not an issue,” he adds.
Dr. Maloney notes that a full list of contraindications has not been developed so far. “We don’t have a lot of data yet,” he explains. “But obviously we don’t implant the Flexivue in patients with keratoconus or significant corneal dystrophies. Also, significant astigmatism is a contraindication because the inlay doesn’t correct astigmatism. We don’t believe the procedure will worsen dry eye because we’re not making a LASIK flap or ablating tissue.”
Nevertheless, Dr. Tamayo believes that patient selection is critical. “In my opinion, a monovision test conducted with a +1.5 D contact lens in the nondominant eye is crucial because it gives the patient the opportunity to experience the controlled monovision the inlay produces,” he says. He adds that the main limitation of the Flexivue may be that monovision effect. “Even though it’s very small, many patients are sensitive to this approach. The rate of rejection after the monovision trial is almost 70 percent.”
Along those lines, some surgeons have patients try bifocal contact lenses before agreeing to implant an inlay, but Dr. Maloney is skeptical about the validity of this approach. “Bifocal contact lenses work in a different way than these inlays,” he notes. “The fact that a patient likes the effect of bifocal contact lenses is no guarantee that he’s going to like the inlay. For example, the Kamra reduces the amount of light coming in because it’s pinhole-based, and it causes some glare because of the 10,000 tiny nutrient holes. A multifocal contact lens doesn’t reduce the incoming light, and any glare it causes would probably be quite different from that caused by the pinholes.”
In any case, Dr. Maloney says the procedure isn’t difficult. “It’s not like mastering cataract surgery, but you do have to be trained in it,” he notes. “For a LASIK surgeon, this will be relatively easy to learn.”
Dr. Tamayo notes that the FDA-approved Phase II clinical studies are just starting.
ReVision Optics’ Raindrop
John A. Hovanesian, MD, clinical assistant professor at UCLA Jules Stein Eye Institute in Los Angeles and in private practice at Harvard Eye Associates in Laguna Hills, Calif., has implanted about 40 of the Raindrop inlays as part of the current United States trial. “I’ve had enough experience to get a pretty good sense of how patients react to it,” he says. “Generally, the reaction is something like the reaction of patients after LASIK—which makes sense because it’s a very similar procedure.
|

Recent data indicates that the Raindrop is effective in a variety of situations, including bilateral implantation:
• Long-term stability. A study by Imola Ratkay, MD, PhD, that will be presented at the 2014 American Society of Cataract and Refractive Surgery meeting, reports two-year visual outcomes with the Raindrop implant in 15 presbyopic patients. Binocular uncorrected near visual acuity improved from 0.22 preop to 0.9 at two years, a gain of six lines; and binocular uncorrected distance visual acuity improved from 0.77 preop to 1.3 at two years. Acuity was stable, tending toward im-provement, and at two years there were no complications.
• Bilateral implantation. A presentation at the 2013 ESCRS meeting reported data from a study in which 23 hyperopic subjects were implanted with the Raindrop bilaterally—first in the nondominant eye, then three to six months later in the dominant eye. Mean near vision improved from 0.54 logMAR to -0.04 logMAR and remained stable; intermediate and distance vision also improved and remained stable. Compared to a single inlay, bilateral implantation added approximately one line of improved near vision. More than 80 percent of the bilateral subjects were 20/20 or better at all distances at all follow-up visits. Task performance improved dramatically at all distances in both bright and dim light. After nine months, all subjects were satisfied with their vision.
• Integrating into a LASIK practice. At this year’s ASCRS meeting Yasuda Kazuomi, MD, will report early results from 107 patients implanted with the Raindrop inlay in the nondominant eye during standard LASIK in Japan. He indicates that he had no trouble integrating the procedure, and patients have achieved good binocular vision, stable refraction and had low rates of complication.
• Cataract surgery after an inlay. Another ESCRS 2013 study reported a case history in which cataract surgery using a femtosecond laser was performed three years after the patient received a Raindrop implant. The surgery was successfully performed with no adjustments to accommodate the implant and no difficulty with measurements or visualization. The patient is happy with the outcome and continues to have a full range of vision.
• Implanting in pseudophakes. Another ESCRS 2013 presentation reported that implanting the Raindrop in the nondominant eye of pseudophakes produced positive results that compared favorably with the results from the multicenter phakic U.S. trial, significantly improving near, intermediate and distance vision.
“The data from outside the U.S. is promising and matches pretty closely what we’re seeing in the U.S. trial,” adds Dr. Hovanesian. “We’re seeing high levels of satisfaction, high levels of spectacle independence and a low level of issues with quality of vision. We’ve seen very few explants or complications.”
The Raindrop in Practice
“Although there’s a little adaptation required, adapting to the Raindrop is a lot easier than adapting to monovision,” notes Dr. Hovanesian. “Many patients can see very well up close and adapt to it right away. Admittedly, these are patients who have been pretested with multifocal contact lenses to prove that they can deal well with this type of refractive change. And that’s an important point: qualifying your patients in advance is a real key to success with an inlay. This is not something you should generally do without trying it first.”
As far as the advantages of this particular inlay, Dr. Hovanesian points out that the Raindrop is very thin and invisible. “The Kamra inlay is very effective, but it’s visible if you look at the eye from the side, particularly if the eye is light-colored, perhaps blue or green,” he says. “Some patients might see this as a disadvantage compared to an implant that’s invisible. Apart from that, it’s difficult to make any comparison, and I don’t think there’s any head-to-head data. Frankly, I’m hopeful that all three of these technologies will gain approval so that we can offer all of them to our patients.”
Regarding contraindications, Dr. Hovanesian says anything that might contraindicate LASIK would also be an issue here. “I wouldn’t use the Raindrop in patients with extremely dry eyes or who have corneal disorders that would make creating a corneal flap or pocket a poor idea,” he says. “These patients need to have good vision in both eyes and be willing to try to adapt to a new optical system.”
Dr. Hovanesian believes the learning curve will be small for most surgeons. “Typically it will be LASIK surgeons doing these procedures,” he says. “As with any new device, there’s a little bit of learning the right way to handle it, but after a few cases with a little bit of guidance almost anybody can do this procedure.”
Dr. Hovanesian adds that the Raindrop inlay is currently in an expansion of the Phase III study. “We’re continuing to collect data, and the data looks good,” he says. “We’re optimistic about the results.”
Closer to a Presbyopia Cure?
“All of these inlays seem to work,” notes Dr. Hovanesian. “You can make theoretical arguments as to why one might be better than the others, but they all seem to achieve a high level of near vision in the range of J1, while only minimally compromising distance vision to 20/20 or 20/25.”
“Overall, the data from the FDA trial of the Kamra, like the data from outside the United States regarding the Flexivue, indicates that these inlays are very safe,” adds Dr. Maloney.
Of course, they have a few disadvantages. Dr. Maloney notes that all of them reduce distance vision to some degree. “That’s the trade-off for improved reading vision,” he says. “And all of them cause night glare to some degree; that’s the trade-off for changing the way the eye focuses light. So if patients aren’t happy, it’s because their night vision isn’t good enough, their distance vision isn’t good enough, or their reading vision isn’t good enough—the inlay isn’t strong enough to give them the reading vision they need. Those limitations are probably common to all inlays. But the inlays can be explanted, and vision returns to being very close to what it was before surgery. In addition, we haven’t seen significant adverse effects with the current generation of these inlays.”
“Using an inlay requires a compromise in distance vision,” agrees Dr. Hovanesian. “That’s the nature of adding something to an emmetropic visual system. However, you’re usually doing it in the nondominant eye in a patient who is a good adapter. For most of these patients, what they sacrifice is well worth it for what they gain.
“The Raindrop inlay, and inlays in general, are going to serve a very important purpose,” he concludes. “As they become approved, we’re going to find that patients really want this kind of technology. It’s appealing because it serves emmetropic presbyopes—patients who are not well served by any other modality we have. Many of these patients are not willing to try monovision, and they’re generally too young for lens implant surgery. They want a quick and easy solution, and they like the idea of something that’s reversible if it doesn’t work out.”
“I think there will definitely be a place for these inlays in our clinical practices,” agrees Dr. Maloney. “It looks like the Kamra inlay is the one closest to FDA approval, but as a surgeon I’d be very happy to add any one of them to my practice.” REVIEW
Dr. Tomita is a consultant for AcuFocus. Dr. Maloney is a paid consultant for Presbia, but has no equity interest or financial incentives relating to the outcome of the Flexivue trial; he has no financial interest in AcuFocus or the Kamra inlay. Dr. Tamayo is a member of the Board of Consultants for Presbia. Dr. Hovanesian is an investigator, consultant and member of the medical advisory board for ReVision Optics, but has no equity interest in the company.
1. Tomita M, Kanamori T, et al. Simultaneous corneal inlay implantation and laser in situ keratomileusis for presbyopia in patients with hyperopia, myopia, or emmetropia: Six-month results. J Cataract Refract Surg 2012;38:495-506.
2. Tomita M, Kanamori T, et al. Small-aperture corneal inlay implantation to treat presbyopia after laser in situ keratomileusis. J Cataract Refract Surg 2013;39:898-905.
3. Waring GO 4th. Correction of presbyopia with a small aperture corneal inlay. J Refract Surg 2011;27:842-5.
4. Seyeddain O, Hohensinn M, et al. Small-aperture corneal inlay for the correction of presbyopia: 3-year follow-up. J Cataract Refract Surg 2012;38:35-45.
5. Chayet A, Garza EB. Combined hydrogel inlay and laser in situ keratomileusis to compensate for presbyopia in hyperopic patients: One-year safety and efficacy. J Cataract Refract Surg 2013;39:1713-21.
6. Garza EB, Gomez S, Chayet A, Dishler J. One-year safety and efficacy results of a hydrogel inlay to improve near vision in patients with emmetropic presbyopia. J Refract Surg 2013;29:166-72.
7. Limnopoulou AN, Bouzoukis DI, et al. Visual outcomes and safety of a refractive corneal inlay for presbyopia using femtosecond laser. J Refract Surg 2013;29:12-8.
8. Jackson GR, Owsley C, McGwin G Jr. Aging and dark adaptation. Vision Res 1999;39:3975-82.
9. King BR, Fogel SM, et al. Neural correlates of the age-related changes in motor sequence learning and motor adaptation in older adults. Front Hum Neurosci 2013;7:142.
10. Yılmaz OF, Alagöz N, et al. Intracorneal inlay to correct presbyopia:Long-term results. J Cataract Refract Surg 2011;37:1275-1281.
11.Alió JL, Abbouda A, et al. Removability of a small aperture intracorneal inlay for presbyopia correction. J Refract Surg 2013;29:8:550-6.