|


The Mechanisms
It is useful to conceptualize the eyelid as comprising three lamellae: 1) anterior—skin and orbicularis muscle; 2) middle—orbital septum and eyelid retractors; and 3) posterior—tarsus and conjunctiva. This model provides a framework for understanding the mechanisms of eyelid malposition and approaches to surgical correction. In general, there are three types of lower eyelid malpositions: entropion; ectropion; and retraction. These are discussed below and summarized in Table 1.
Numerous factors interplay to influence eyelid position and orientation. For example, horizontal laxity may destabilize the lower eyelid, causing the eyelid to turn outward or inward, depending on anatomic comorbidities, such as deficiency of the anterior or posterior lamella, prominence of the globe and orbicularis oculi muscle tone. Examination should document the lower eyelid margin and punctal position, degree of eyelid laxity (by the eyelid distraction test), orbicularis tone (by the “snap test”), orbicularis muscle strength (on forced eyelid closure), and size of the tear lake, in addition to any trichiasis and exposure keratoconjunctivitis.
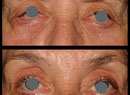
On the snap test, when the lower eyelid is everted in the presence of normal muscle tone, the eyelid should return to its proper position against the globe within a second or two, even without an eyelid blink. If there is poor muscle tone, which may be found with facial nerve palsy, myopathy or advanced age (See Figure 1), the lower eyelid slowly swings back against the globe, taking several seconds or awaiting a blink to pull the eyelid inward. A lax lower eyelid with poor orbicularis muscle tone tends to swing outward, away from the globe, succumbing to the effect of gravity, resulting in ectropion.
|
Entropion
Entropion is characterized by inward rotation of the eyelid margin (See Figure 2), which may result in pain and corneal injury.
The etiology may be involutional, cicatricial, spastic or, rarely, congenital. Involutional entropion typically involves horizontal eyelid laxity with dehiscence of the eyelid retractors and override of the preseptal over the pretarsal orbicularis oculi muscle. Spastic entropion is due to excessive contraction of the orbicularis muscle. Cicatricial entropion (See Figure 3) involves a tight posterior lamella due to scarring of the conjunctiva and/or tarsus. This scarring may result from trauma, surgery, or cicatrizing conjunctivitis due to infection (e.g., trachoma), topical medications (pseudopemphigoid), or a systemic disorder such as ocular cicatricial pemphigoid (OCP) or Stevens-Johnson syndrome. The etiology of the entropion must be understood before proceeding with treatment, as it will impact the choice and timing of surgery. For example, OCP must be treated with systemic immunomodulatory therapy before surgery. Cicatricial entropion usually displays visible conjunctival scarring and/or symblepharon, altered eyelid margin architecture and characteristic response to digital eyelid eversion. With involutional entropion, if you evert the eyelid to its proper anatomic position, it will usually stay in this position for at least a few seconds after releasing the eyelid, often until the patient blinks. With cicatricial entropion, when the eyelid is released, it promptly turns inward again.
|

Regarding treatment of entropion, everting (Quickert) sutures may be used. This consists of placing three horizontal mattress sutures (medially, centrally and laterally, with all sutures lateral to the punctum) from the inferior conjunctival fornix out through skin just below the lash line. The lower the sutures are placed in the fornix, and the closer they are to the lash line as they exit the skin, the greater the everting effect. Everting sutures are quite effective as a temporary measure, but are generally not believed to provide long-term correction. Taping of the lower eyelids is often used for elderly patients, although this is difficult to do effectively and may cause skin irritation. Botulinum toxin injections may have a role in spastic entropion.
Numerous surgical procedures have been reported for repair of entropion. For involutional entropion, successful corrective surgery usually combines horizontal tightening of the eyelid (usually via the lateral tarsal strip procedure), advancing the lower eyelid retractors, and, when needed, the creation of a full-thickness eyelid scar to prevent the preseptal orbicularis muscle from overriding the pretarsal muscle. Recent reports suggest that the combination of horizontal eyelid tightening and Quickert sutures can be quite successful in involutional entropion.
| ||||||


Ectropion
Ectropion denotes outward rotation of the eyelid margin (See Figure 4). The etiology may be classified as involutional, cicatricial, paralytic, mechanical or congenital. Mechanical ectropion can be seen when the lower eyelid is very swollen or there is a large mass lesion, particularly in the face of severe horizontal eyelid laxity. Cicatricial ectropion may result from skin shortage and/or scarring, e.g., due to surgery, trauma, sun damage or chronic dermatitis. Congenital ectropion often shares with cicatricial ectropion the common factor of skin shortage. Facial nerve palsy often results in paralytic ectropion (See Figure 5), particularly in the elderly. Ectropion may produce exposure keratoconjunctivitis and/or tearing. Both entropion and ectropion may cause inferior corneal ulceration, which is an urgent indication for surgical repair.
|

Lower Lid Retraction
Lower lid retraction (See Figure 6) is commonly defined as a lid margin position below the inferior limbus (inferior scleral show). There is a broad differential diagnosis for eyelid retraction, and this has been well-reviewed by George Bartley, MD.1 Thyroid eye disease is, by far, the most common cause of eyelid retraction, although non-thyroid proptosis, severe lid laxity or eyelid scarring may also be responsible. The appropriate treatment depends on the underlying cause. In the case of thyroid eye disease, non-urgent surgery should usually be delayed until the eye condition is stable and inactive. Involutional retraction (sagging) of the lower eyelid may result from horizontal eyelid laxity, while cicatricial retraction results from scarring in the middle lamella (lower eyelid retractors and orbital septum).
Regarding treatment, hyaluronic acid dermal filler injection has been shown to modestly improve lower eyelid retraction, as a nonsurgical alternative in patients with exposure keratopathy due to eyelid retraction. The nature of the surgical repair undertaken depends upon the cause of the retraction. In the case of a lax, sagging lower eyelid, horizontal tightening should be sufficient. If the lower eyelid retractors are tight, then they should be recessed. If the globe is proptotic, then either supra-placing the lateral canthal angle or placing a rigid spacer graft, e.g. hard palate, in the middle lamella of the lower eyelid will be required. Any scar tissue contributing to the eyelid retraction, such as fibrosis to the inferior orbital rim or an alloplastic plate following orbital floor fracture repair, should be surgically divided. A temporary Frost suture, placing the lower eyelid on upward stretch, is commonly employed following surgery.
Lower eyelid malposition is commonly encountered in clinical practice. Symptoms can range from none to tearing or severe pain. Patients can develop vision-threatening sequellae, such as a corneal ulcer, and they may have an underlying systemic disorder. Prompt evaluation and management will protect the eye and allow early detection of an underlying systemic medical condition. REVIEW
Dr. Weinberg is in private practice in Concord, N.H.
1. Bartley GB. The differential diagnosis and classification of eyelid retraction. Ophthalmology 1996;103:168-76.
2. Bleyen I, Dolman PJ. The Wies procedure for management of trichiasis or cicatricial entropion of either upper or lower eyelids. Br J Ophthalmol 2009;93:1612-5.
3. Chung JE, Yen MT. Midface lifting as an adjunct procedure in ectropion repair. Ann Plast Surg 2007;59:635-40.
4. Elner VM, Demirci H, Morton AD, et al. Transcaruncular medial canthal ligament plication for repair of lower eyelid malposition. Arch Ophthalmol 2007;125:374-9.
5. Erb MH, Uzcategui N, Dresner SC. Efficacy and complications of the transconjunctival entropion repair for lower eyelid involutional entropion. Ophthalmology 2006;113:2351-6.
6. Goldberg RA, Lee S, Jayasundera T, et al. Treatment of lower eyelid retraction by expansion of the lower eyelid with hyaluronic acid gel. Ophthal Plast Reconstr Surg 2007;23:343-8.
7. Jordan DR, Anderson RL. The lateral tarsal strip revisited. The enhanced tarsal strip. Arch Ophthalmol 1989;107:604-6.
8. Kirzhner M, Jakobiec FA. Ocular cicatricial pemphigoid: A review of clinical features, immunopathology, differential diagnosis, and current management. Semin Ophthalmol 2011;26:270-7.
9. Nowinski TS, Anderson RL. The medial spindle procedure for involutional medial ectropion. Arch Ophthalmol 1985;103:1750-3.
10. Oestreicher JH, Pang NK, Liao W. Treatment of lower eyelid retractor release and posterior lamellar grafting: An analysis of 659 eyelids in 400 patients. Ophthal Plast Reconstr Surg 2008;24:207-12.
11. Rougraff PM, Tse DT, Johnson TE, Feuer W. Involutional entropion repair with fornix sutures and lateral tarsal strip procedure. Ophthal Plast Reconstr Surg 2001;17:281-7.
12. Steel DH, Hoh HB, Harrad RA, Collins CT. Botulinum toxin for the temporary treatment of involutional lower lid entropion: A clinical and morphological study. Eye (Lond) 1997;11:572-5.