Glaucoma drainage devices have become more frequently used to treat glaucoma that’s refractory to maximum tolerated medical therapy. This is following the results of the Tube Versus Trabeculectomy study, which reported better success at five years with Baerveldt implantation than with trabeculectomy with mitomycin-C in patients who had undergone previous surgery. A follow-up Primary Tube Versus Trabeculectomy study is under way to assess the efficacy of Baerveldt implantation in patients without previous surgery. In addition, two major trials are comparing the two most commonly used glaucoma drainage devices (the Ahmed and Baerveldt implants): the Ahmed Versus Baerveldt study (which we are involved in) and the Ahmed Baerveldt Comparison study.
AVB at Year Three
Last November we presented the three-year results of the Ahmed Versus Baerveldt study, an international, multicenter, randomized trial of 238 patients with uncontrolled or high-risk glaucoma, at the American Academy of Ophthalmology Annual Meeting. Enrolled patients had failed to achieve target pressures despite maximum medical therapy, and many had already failed trabeculectomy and/or trabeculoplasty. Mean preoperative IOP was 31.4 ±10.8 mmHg on 3.1 ±1.0 glaucoma medications with a median Snellen visual acuity of 20/100.
|
In brief, the three year data showed that:
• Both devices were effective in reducing IOP and the need for glaucoma medications.
• The cumulative probability of failure was significantly greater in the Ahmed group (51 percent, vs. 34 percent in the Baerveldt group; p=0.03).
• Mean IOPs at three years were not significantly different, although there was a trend toward a lower IOP in the Baerveldt group (14.4 ±5.1 mmHg vs. 15.7 ±4.8 in the Ahmed group, p=0.09).
• Fewer medications were required in the Baerveldt group (1.1 ±1.3 vs. 1.8 ±1.4 in the Ahmed group; p=0.002).
• Complication rates were not significantly different, but the Baerveldt group had a higher rate of hypotony-related, vision-threatening complications (6 percent vs. 0 percent in the Ahmed group; p=0.005). Also, there was a trend towards more interventions being required in the Baerveldt group, although most interventions were only slit-lamp procedures. Both groups had a moderate decrease in visual acuity.
Overall, both of these devices were effective treatment options, even in this population of challenging patients. The Baerveldt had a higher success rate and required fewer medications, but had a higher rate of serious hypotony-related complications. These results are not entirely surprising; the ABC study reported similar findings.
Choosing a Shunt
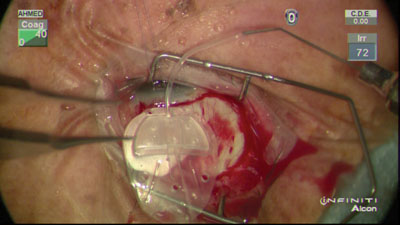
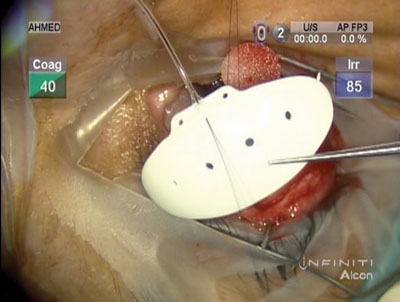
Selecting a device involves balancing many factors, including a patient’s age, glaucoma subtype and treatment goals. For example, although the Baerveldt may yield a lower long-term pressure (note that the difference was not significant in our trial), there is often pressure volatility in the early postop period that may not be amenable to patients with severe disease. Because the Baerveldt tube is occluded during the first four to six weeks after surgery while the bleb forms around the plate, it often requires manipulation and intervention. However, this appears to have a long-term beneficial effect on the bleb; it’s not exposed to early postop aqueous that may cause inflammation and bleb remodeling. Eventually, when the tube occlusion dissolves or is removed, flow begins. That can cause the pressure to drop quickly and may result in hypotony-related complications, the major risk associated with this device. In contrast, the Ahmed has a built-in valve mechanism that allows immediate postoperative flow and prevents hypotony, but may require more glaucoma medications in the long term.
Some people might interpret our results to mean that the Baerveldt is a better device than the Ahmed, but which device is “better” depends on the situation. Treating glaucoma is about individualizing patient care by using your clinical acumen to determine treatment goals.
For example, if I need to get a patient’s pressure as low as possible to prevent progression, I might choose a Baerveldt device. If I’m trying to treat somebody with a higher target pressure or with neovascular glaucoma and I just want to get the pressure down to a more normal level, then I might choose an Ahmed valve because the risk to the patient is less. If I have a patient younger than 50 years old, which would make me concerned about healing and bleb encapsulation, then I’d probably choose the Baerveldt. If a patient is over 75 and just had surgery, I’d prefer the Ahmed for safety reasons, and perhaps because of life expectancy. If a patient has had a failed trabeculectomy and we’ve needled the bleb and it’s scarred down, and the conjunctiva isn’t in great health, I’d probably consider a Baerveldt.
Sadly, we’ve seen very little innovation in the area of glaucoma drainage devices. There are a few alternatives to the Ahmed and Baerveldt devices such as the Molteno 3 device and the Krupin device, but they’re not new and they’re not used as often. A device with some sort of flow control would be excellent, but that hasn’t appeared yet. However, many new devices are allowing us to increase drainage into other spaces, including Schlemm’s canal and the choroidal space. Many of the procedures surrounding those devices are less invasive and easier to accomplish.
Turning to MIGS?
That raises the issue of the increasingly popular minimally invasive glaucoma surgeries, including placement of the iStent in Schlemm’s canal. This may not seem like a fair comparison, because generally these procedures are thought of as treatments for mild to moderate glaucoma. Typically, the patients who undergo these procedures have healthier eyes, and these procedures are more often combined with cataract surgery. In contrast, the glaucoma drainage devices are generally reserved for more advanced patients with sick eyes and multiple risk factors; they’re less often combined with phaco and may involve multiple surgeries with a complicated postoperative course.
Nevertheless, the idea of using some of these devices to treat more advanced patients is gaining credibility, at least in my experience. For example, I recently had a challenging monocular 70-year-old patient with a failed trabeculectomy. We had done needling, but his pressure was still at 24 mmHg on four medications. And, he had a cataract. Many surgeons would have opted for a tube or a second trab, and the TVT study might have inclined the surgeons to choose a Baerveldt.
However, in this case I was very concerned about the risks. I talked with the patient extensively, and we eventually agreed to try doing phaco with the implantation of multiple iStents (with the option of going to a tube later, if required). We felt that there was a chance this might work, and if it did, it would save the patient from having to undergo a riskier procedure. To maximize the odds of a good outcome, when it came time to do the surgery we used our “targeted” approach, in which we place the iStents in areas of high capacity, near aqueous veins.
The patient is currently four months out. To our amazement, his pressure is now hovering around 13 mmHg—on no glaucoma medications. That’s a home run, which we don’t always manage to achieve. But if we can reach that level of success with this kind of patient, then MIGS may have more potential than many surgeons currently believe. We definitely need to learn more about these devices and procedures and how to use them most effectively.
I think that all surgeons are capable of performing the MIGS procedures. However, these procedures are highly technical. I’ve been doing them for six years now, and it’s taken me that long to feel that I know their nuances, including the technical planning and patient indications. As a result, I’m definitely hitting more home runs with these procedures today than I did early on.
I’m really excited about these procedures, and I’m looking forward to seeing their role expanded. I believe these procedures will eventually be chosen for some of the patients who currently are seen as candidates primarily for tubes or trabs. (For more on the MIGS procedures, see “MIGS and the General Ophthalmologist” on p. 34.)
Whether you choose to resort to a trabeculectomy, a tube or one of the newer MIGS procedures when faced with a challenging case, there’s no question that it’s an exciting time to be a glaucoma surgeon. Technological innovation and research are thriving in the field. We hope that this will translate into better outcomes for our patients. REVIEW
Dr. Ahmed is an assistant professor at the University of Toronto in Ontario. (He is not the creator of the Ahmed valve and has no financial interest in it.) Dr. Christakis is an ophthalmology resident at the University of Toronto.


