Presentation
An 11-year-old boy presented to the Wills Eye Hospital Emergency Room, referred from an outside hospital, with photophobia, redness and decreased vision in his left eye for three days. He had only mild eye pain. Two CT scans of the brain and orbits done in the days prior to referral were normal. The patient and family denied any ocular trauma, recent travel or disease contacts. The patient had vague, non-specific left leg pain without a limp. Review of systems was otherwise negative.
Medical History
|
Examination
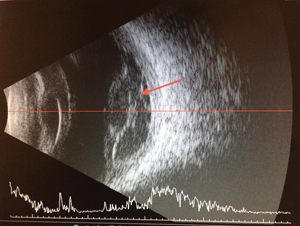
Ocular examination revealed a visual acuity of 20/20 in the right eye and light perception in the left eye. The left pupil was slightly irregular and nonreactive with an afferent pupillary defect. Goldmann applanation tonometry was 10 and 11 mmHg. Extraocular movements were full in both eyes, and there was no pain with movement. Confrontation field testing was full in the right eye and limited by the poor visual acuity in the left eye. External examination was significant only for mild lid edema and erythema of the left eye. Slit-lamp examination of the right eye was unremarkable. The left eye had moderate conjunctival injection without chemosis, minimal corneal stromal haze, moderate anterior chamber cell and a disc of fibrin in the anterior chamber overlying the pupil. The lens was clear. Dilated fundus examination of the right eye was normal. There was no view of the left eye due to white retrolental material. B-Scan ultrasound (See Figure 1) showed intense cellular debris in the vitreous, thickening of the choroid and thin vitreous membranes.
What is your differential diagnosis? What further workup would you pursue?
Please click this link for diagnosis, workup, treatment and discussion.


