This month we’ll take a closer look at AIT, examine prospects for an immunization approach to treatments for ocular allergy and discuss how current and future clinical trials might be optimized for AC indications.
Turning Off the Allergic Switch
Use of plant or pollen extracts to reduce signs and symptoms of “hay fever” dates back to the early 20th century.1 It’s interesting that despite this long history of AIT for rhinitis, the use of such treatments specifically for AC is much less common. This trend appears to be shifting, with the recent publication of Phase III studies of tablet formulations for AIT therapy of either grass- or ragweed-evoked allergy. In both cases the indications for each treatment are the same: “rhinitis with or without AC.”2,3
Allergic conjunctivitis is one of several related disorders that involve development of a Th2 T-cell response to common environmental allergens, leading to activation of antigen-specific IgE production and immunological sensitization.4,5 When these sensitized individuals are subsequently exposed to the allergenic culprit, antibodies can initiate mast cell degranulation and the subsequent sequelae of an allergic response (See Figure 1).
|
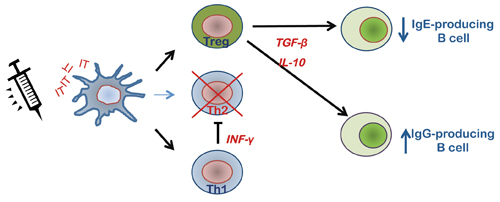
Now, if dendritic cells or other antigen-presenting cells are repeatedly exposed to the same antigen (particularly at low concentrations), it’s possible to initiate a shift in the regulatory balance between the Th2 pathway and the non-allergenic Th1/T0-based signaling paradigm.4,5 Although this desensitization process is not completely understood, increases in IL-10, TGF-β and INF-γ promote a conversion from IgE to IgG antibody production, a suppression of inflammatory leukocytes and an attenuation of subsequent responses to allergen exposure.
This all sounds so good, one might wonder why immunotherapy isn’t a mainstay of allergy therapy. It seems there are limitations to the utility of this treatment, and these, along with the availability of simpler remedies, have slowed the rush towards AIT.
Holding Back on AIT
The current therapeutic approach to ocular allergic disease is dominated by topical and systemic antihistamines, agents that have evolved to once-daily treatments that provide effective symptomatic relief to a large proportion of those with AC. Unfortunately, for 25 to 35 percent of the 40 million people in the United States with seasonal or perennial allergy, these traditional treatments provide little or no relief.6 For these patients, AIT is a natural option that has the potential to provide a safe, long-lasting mitigation of allergic symptomatology. Despite this, its use has been constrained by a number of factors.
Most AIT protocols employ a single antigen, even though patients are often allergic to multiple antigens such as pollens of grass, ragweed or birch. This means patients must go through multiple treatments for each allergen, or undergo treatment with allergen mixtures prepared on-site or by compounding pharmacies. Standards adopted by U.S. Pharmacopeia and professional associations such as the American Academy of Allergy, Asthma & Immunology include the option of subcutaneous injection of allergen mixtures, but these present a new set of roadblocks.7 Often allergens have inherent proteolytic activity that can lead to reduction or elimination of antigenicity, especially in mixtures. In addition, despite the establishment of these standards, there are few controlled studies confirming the efficacy of mixed-allergen immunotherapy. Published clinical trial data are mostly based upon studies from Europe, where there is a greater emphasis on monotherapy using European Medicines Agency approved formulations.7,8
Another issue that has hindered development of AIT is safety concerns regarding risk of anaphylaxis. This is probably the most important reason that sublingual formulations, either liquid or tablet, are not approved for use in the United States.9 As the number of studies has grown, however, it appears that such concerns may have been overstated; the incidence of anaphylactic reactions in clinical trials is extremely low.10 In addition, a review of 11 case reports of anaphylaxis associated with AIT found that each corresponded to non-standard practice or protocol deviation, and none of these reported cases involved a fatality.11 When properly used, it appears that AIT has an excellent margin of safety.
Other issues may also play a part in the limited inroads of AIT in treatment of ocular allergy. There is a belief that AIT requires a long duration of therapy before significant relief can develop, even though most studies have shown a reduction in allergic symptomology within weeks of therapy initiation.12 One factor that still appears unresolved is how different dosing regimens should be developed and validated. Perhaps most important is that despite the high numbers of recent trials using grass, ragweed and dust mite AIT, very few of these studies explicitly addressed ocular signs and symptoms. Without such objective metrics it’s hard to judge whether a given treatment specifically addresses the needs of patients with AC.
Sublingual Immunotherapy
We mentioned earlier that, in the United States, virtually all immunotherapy employs subcutaneous injection as the route of administration, making the need for repeated office visits a major impediment to growth of this therapy. It’s fair to say that the reason AIT is so much more common in the EU compared to the United States is the availability of oral and topical delivery formulations of antigen.9 Both of these treatment modalities have shown similar efficacy and safety profiles when compared to subcutaneous antigen delivery. Recent large-scale trials in the United States have focused on sublingual immunotherapy, or SLIT, a modality that has the potential to expand the use of AIT to a much greater patient population.2,3 Despite this advance, most of these trials haven’t addressed the efficacy of SLIT in relief of ocular allergy.
Patients with allergies commonly experience a spectrum of symptoms that includes ocular itching, hyperemia and chemosis. More than 80 percent of allergy sufferers report experiencing some ocular symptomology,13 yet the latest trials in the United States have been environmental exposure-based studies that provided only limited measures of ocular symptoms as part of a six-part composite score. This daily symptom score included values for “gritty/itchy/red eyes” or “teary/watery eyes.”2,3 Such categories don’t reflect an accurate measure for AC, and can be impacted by conditions other than allergy. In these and other recent trials, no scores providing a direct measure of ocular itching are collected.
Most trials also lack a positive comparator group such as antihistamine or steroid therapy (though such controls would present problems to blinding). The second scoring metric in these studies is a daily medication score (including eye drops) that affords some evidence of ocular efficacy, but doesn’t provide a comparison between AIT and established allergy treatments. Overall, flaws in study design may be a reflection of the low statistical power inherent in all environmental trials.14
Environmental trials depend upon naturally occurring levels of antigen, and thus may tend to underreport the effectiveness of a given test treatment. We’ve shown the unique value of allergen-challenge based trials for development of therapeutics for ocular allergy over more than 30 years of studies. An approach similar to the conjunctival allergen challenge methodology is likely to provide a rapid, accurate assessment of AIT efficacy in treatment of both ocular and nasal symptoms.
As a strategy to validate AIT, provocation tests have already been shown to provide a reliable metric of therapeutic efficacy. In an early trial of birch pollen AIT, subjects received a 28-day course of allergen followed by a three-month maintenance treatment.15 Evaluation before and after treatment (four months after the last maintenance dose) was by skin-prick and conjunctival provocation test in a dilution series to determine the threshold of allergic sensitivity. Patients also underwent a two-hour exposure to birch pollen in a chamber. Following AIT treatment, the amount of allergen required to elicit symptoms in the conjunctival provocation that were comparable to the pre-AIT response was significantly increased. The skin test and nasal assessments also showed statistically significant improvements from AIT compared to placebo. While the number of such studies is low, they all demonstrate the utility of a provocation test alternative to environmental exposure-based trials for assessment of AIT.
The few studies that include conjunctival challenge data suggest that ocular itching may be a more sensitive measure of efficacy than environmental symptom scores alone. In a recent report, ocular itching was reduced 30 to 48 percent from placebo, while the threshold for conjunctival response to allergen provocation was significantly increased.16 When compared to the best reported nasal or ocular symptom score improvements of 24 to 28 percent, it seems that some of these early studies may have omitted a valuable endpoint from their trials.
Allergen challenge has been used to measure efficacy of allergen desensitization, and can provide an objective measure of the treatment effects on either nasal or ocular symptoms. In addition, conjunctival allergen challenge protocols such as the CAC are validated metrics that provide established endpoints for Food and Drug Administration assessment of AC therapies. Metrics like the CAC have not been employed to develop new AIT-based therapies to date, but we think they should be. If we are to fight fire with fire, it’s especially critical to employ the best possible tools to gauge our progress, because we’ll never know the battle is won unless we keep our eyes open. REVIEW
Dr. Abelson is a clinical professor of ophthalmology at Harvard Medical School. Mr. Gomes is vice president of allergy at Ora; Dr. McLaughlin is a medical writer at Ora Inc.
1. Noon L. Prophylactic inoculation against hay fever. Lancet 1911;1:1572–3.
2. Maloney J, Bernstein DI, Nelson H, et al. Efficacy and safety of grass sublingual immunotherapy tablet, MK-7243: A large randomized controlled trial. Ann Allergy Asthma Immunol 2014;112:146-153.
3. Creticos PS, Maloney J, Bernstein DI, et al. Randomized controlled trial of a ragweed allergy immunotherapy tablet in North American and European adults. J Allergy Clin Immunol 2013;131:1342–1349.
4. Fujita H, Soyka MB, Akdis M, Akdis CA. Mechanisms of allergen-specific immunotherapy. Clin Transl Allergy 2012;2:2.
5. Nelson HS. Subcutaneous Injection Immunotherapy for Optimal Effectiveness. Immunol Allergy Clin N Am 2011;31:211-226.
6. Blaiss MS. Allergic rhinoconjunctivitis: Burden of disease. Allergy Asthma Proc 2007;28:393–397.
7. Cox L, Esch RE, Corbett M, et al. Allergen Immunotherapy Practice in the United States: guidelines, measures, outcomes. Ann Allergy Asthma Immunol 2011;107:289-301.
8. Cox L, Jacobsen L. Comparison of allergen immunotherapy practice patterns in the United States and Europe. Ann Allergy Asthma Immunol 2009;103:451-460.
9. Nelson HS. Is sublingual immunotherapy ready for use in the United States? JAMA 2013:309;1297-98.
10. Lin SY, Erekosima N, Kim JM, et al. Sublingual Immunotherapy for the Treatment of Allergic Rhinoconjunctivitis and Asthma. A Systematic Review JAMA 2013;309:1278-1288.
11. Calderon MA, Simons FE, Malling HJ, Lockey RF, Moingeon P, Demoly P. Sublingual allergen immunotherapy: Mode of action and its relationship with the safety profile. Allergy 2012;67:302.
12. Calderón MA, Frankland AW, Demoly P. Allergen immunotherapy and allergic rhinitis: False beliefs. BMC Med 2013;11:255.
13. Tan BK, Chandra RK, Pollak J. Incidence and associated premorbid diagnoses of patients with chronic rhinosinusitis. J Allergy Clin Immunol 2013;131:1350-1360.
14. Abelson MB. Comparison of the conjunctival allergen challenge model with the environmental model of allergic conjunctivitis. Acta Ophthalmol Scand Suppl 1999;228:38-42.
15. Horak F, Stübner P, Berger UE, Marks B, Toth J, Jäger S. Immunotherapy with sublingual birch pollen extract. J Invest Allergol Clin Immunol 1998;8:3:165-71.
16. Calderon MA, Penagos M, Sheikh A, Canonica GW, Durham SR. Sublingual immunotherapy for allergic conjunctivitis: Cochrane systematic review and meta-analysis. Clin Exp Allergy 2011;41:1263-72.


