Three main techniques are currently used to treat RRD: 1) scleral buckle surgery; 2) pars plana vitrectomy with retinopexy and intravitreal tamponade1,2,7; and 3) pneumatic retinopexy. Studies have generally failed to show superior anatomic or visual outcomes with one technique over another.1 The choice of technique comes down to a combination of surgeon experience and preference, the nature and extent of RRD, and the number, distribution and type(s) of retinal break(s).
While there has been a shift over the past two decades toward PPVs,8,9 in our opinion, primary SB remains the treatment of choice for certain RRD types, particularly in eyes without an existing posterior vitreous detachment.10 The techniques of SB surgery have remained largely unchanged for the past 50 years. The goal is to create an inward indentation of the eye wall, thus approximating the retinal pigment epithelium to the neuroretina surrounding the break. Scleral indentation is achieved by the placement of a permanent episcleral explant/buckle at a location corresponding to the retinal break. The buckle is permanently anchored to the sclera, typically with non-dissolvable sutures. Buckle materials include silicone sponge and hard silicone that come in a variety of shapes and sizes. The exact type of buckle required varies according to the desired buckle (scleral indentation) height, and location and number of breaks.
|
Retinal Detachment
Rhegmatogenous retinal detachment occurs when there is a full-thickness break in the retina, together with a change in the balance of forces favoring neurosensory retinal detachment from the underlying RPE, over physiologic attachment. Importantly, three types of retinal breaks can occur, which can influence the choice of surgical procedure: 1) tear (also known as flap, horseshoe or U-tear); 2) round hole (also known as atrophic holes); and 3) dialysis.
The most common mechanism of RRD is the formation of a full-thickness retinal tear during the development of a PVD.1,10 Retinal tears account for 90 percent of RRDs, resulting from the traction exerted on the peripheral retina by the posterior hyaloid face, typically at the posterior border of the vitreous base.8
Round holes develop as a result of intraretinal abnormalities or in areas of lattice degeneration, and are more common in myopic eyes. For reasons that remain unclear, most round holes do not lead to retinal detachment.
Retinal dialyses occur when the retina detaches from its insertion at the ora serrata together with the vitreous base—often following blunt ocular trauma.12 A PVD is typically absent unless pre-existing.
With all of the above break types, a full thickness retinal hole enables liquefied vitreous to flow into the subretinal space, separating the neurosensory retina from the RPE.10,11 Although the initial presentation of patients with symptomatic detachment does vary, common symptoms include:
• PVD-related photopsias (flashing lights);
• a sudden increase in vitreous floaters, due to release of RPE cells and/or blood into the vitreous cavity;
• visual field defects; and
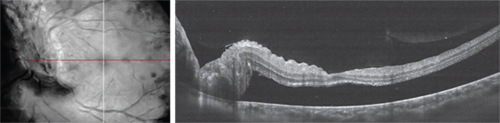
• decreased visual acuity-RRD involving the macula.
Surgical Outcomes
Post-surgical visual outcomes relate to the extent of initial macular involvement.13 The retina is reattached in 90 percent of cases, with success rates nearing 100 percent in certain case series.1 However, there is a significant difference between favorable anatomic correction and functional visual outcomes. The presence of macular involvement (“macula-off” RRD) is the most important issue when it comes to success in restoring visual acuity.13
|
The main factors predicting poorer visual function after surgery include:
• poor preoperative visual acuity (reliable predictor);14
• increasing extent (clock hours) of RRD;
• increasing number of retinal breaks;
• inferiorly positioned breaks;
• macula-off (or macular-involving) RRD;
• preoperative proliferative vitreoretinopathy of any grade (PVR); and
• intraoperative hemorrhage.
Indications for SB Surgery
While PPV and pneumatic retinopexy are increasingly used for the repair of uncomplicated RRD, SB surgery still has an important role in certain RRD types.8,10,15 In some cases, vitreous surgery is necessary to relieve vitreoretinal traction that cannot be adequately relieved by scleral buckling and other conventional retinal reattachment techniques.
In our experience, SB is the treatment of choice in patients with uncomplicated RD, in retinal dialysis and for RRDs associated with round holes.
Combined PPV+SB surgery may be associated with a decreased risk for retinal redetachment when compared to PPV for repair of phakic RRD, especially in cases with severe PVR, inferior traction and with incomplete removal of traction. The improved success rate is contributing to the function of vitrectomy, which improves peripheral visibility and reduces the occurrence of proliferative vitreoretinopathy. Some studies showed that in pseudophakic eyes, the anatomic success rate between PPV and combined PPV+SB techniques appears to be similar.16,17
In summary, RRDs with any of the following features can benefit from SB surgery:
• no posterior vitreous separation (no PVD): it could be hard to induce a PVD and remove the posterior vitreous in an eye with an RD;
• dialysis: usually no PVD and hard access to the periphery with PPV in a phakic eye (lens touch);
• round or atrophic holes;
• breaks anterior to the equator: easy to place a buckle in the right position and hard access to the periphery with PPV in a phakic eye (lens touch);
• inferior breaks: support of the vitreous base or peripheral retina; and
• certain complex retinal detachments with PVR: 360-degree support of the vitreous base or peripheral retina.
There are three main SB techniques, namely: 1) encircling circumferential buckle; 2) segmental/limited circumferential buckle; and 3) radial buckle. The choice of technique relates in part to surgeon preference and experience, and there is wide international variation.
Encircling buckles confer a permanent 360-degree scleral indent and may be used in cases where there is concern about potentially unidentified and untreated breaks. There is, however, a greater risk of buckle intrusion and anterior segment ischemia with encircling as compared to segmental buckles.
| ||||||
Radial buckles with a sponge are best for single breaks between recti muscles (for easiest access), particularly highly elevated retinal tears.
Surgical Technique
Scleral buckle surgery can be easily summarized into several discrete steps, as follows:
1. Conjunctival peritomy and isolation of rectus muscles.
2. External localization of all retinal breaks.
3. Decide on buckle type and location.
4. ±External drainage of subretinal fluid.
5. Treat break(s)—cryotherapy, typically.
6. Place and secure buckle.
7. Retinal examination.
8. Conjunctiva and Tenon’s capsule closure followed by subconjunctival steroid and antibiotic injection.
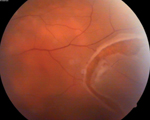
However, there are important pearls and pitfalls to bear in mind to optimize the chance for success. The most important aspect of any approach to treating RRD is the ability to localize and treat all retinal tears (See Figure 2), without which any technique is far more likely to fail. Preoperative assessment and planning is the key to success in SB surgery. Evaluate using an indirect ophthalmoscope with a condensing lens (20 or 28D), preferably with scleral indentation to optimize the view of the peripheral retina. If the view of the retina is compromised by media opacities, e.g., vitreous hemorrhage, such that the ability to adequately perform SB is compromised, PPV should be considered.1,18,19
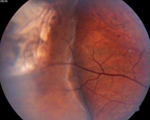
Once all the breaks have been localized and marked appropriately, retinopexy is typically performed with cryotherapy (See Figure 3). It is difficult to achieve adequate retinopexy with laser photocoagulation alone in the presence of even shallow subretinal fluid.
Drainage of the subretinal fluid may be required in the following situations:
• highly elevated break and detachment precluding adequate cryotherapy to retinal break;
• high scleral indentation of more than six clock hours required subsequent intraocular pressure rise sufficient to occlude central retinal artery despite repeated paracentesis; and
• chronic detachments.
Techniques for external drainage of subretinal fluid include a needle drain and scleral cut down with choroidotomy (laser or needle). Our preference is for a needle drain technique. A spatulated needle with an exposed 2- to 2.5-mm tip is used to create a single stab into the sclera at a site with deep subretinal fluid (elevated retina a long distance away from the RPE). Constant firm external pressure is applied on the globe for several minutes to encourage subretinal fluid egress. If drainage is planned, it is wise to pre-place scleral sutures for the buckle, as suturing the sclera in a hypotonous eye is challenging with an increased risk of choroidal hemorrhage.
If a non-drainage technique is chosen, it may be necessary to do an anterior chamber paracentesis to lower IOP, which may be repeated.
The choice of buckle depends on a number of factors, principally the number and location of breaks and desired height of scleral indentation. The choice of encircling versus segmental versus radial buckles has been discussed in the previous section. Explants come in a variety of shapes and sizes. A buckle of sufficient width must be chosen to ensure the buckling element and indent extends past the posterior portion of the retinal break (See Figure 3). Accurate break localization, noting the most posterior extent, is essential. For example, with a large retinal dialysis, the most posterior edge of the dialysis can hang back a surprisingly long way from the ora serrata; a buckle of sufficient width needs to be chosen to provide indentation from the ora serrata to the posterior limit of the dialysis.
Finally, examine the fundus with an indirect ophthalmoscope to confirm that the break is fully supported by an adequate indentation without fish mouthing, and to ensure that the central artery is patent.
Contraindications/Complications
A SB is contraindicated in the following scenarios:
• detachments caused by breaks significantly posterior to the equator; these may be technically difficult to repair using a buckle;
• opaque media (e.g., vitreous hemorrhage);
• significant vitreoretinal traction (such as with PVR and diabetic neovascularization): a PPV approach is usually favored.20-22
The potential intra- and postoperative complications of SB surgery are relatively small. The main risks are:
• anatomical failure (e.g., inadequate buckle height, missed breaks and PVR);
• immediate and early postoperative discomfort;
• refractive error, strabismus and double vision;
• glaucoma;
• choroidal hemorrhage;
• buckle infection (now very uncommon with closed rather than opened air cell sponges being used);
• extrusion of the buckle; and
• anterior segment ischemia.
Occasionally scleral buckles need to be removed because of complications, as highlighted above.23,24
The surgical treatment for RRD depends largely upon surgeon experience and preference.25,26 While PPV has been used routinely to treat RRD of all types in recent years, our preference is to use SB surgery for certain RRD break types—specifically round holes and dialyses in the absence of a PVD. REVIEW
Dr. Sabrosa is a retinal specialist in Rio de Janeiro, Brazil. He was a surgical retina fellow at Moorfields Eye Hospital (UK) and is now director of the Medical Retina and Vitreoretinal Services at Santa Casa de Misericordia do Rio de Janeiro (1ª Enfermaria), and is in private practice at Clínica São Vicente, Rio de Janeiro. Contact Dr. Sabrosa at Clínica de Olhos Gávea, Rua João Borges, 204, Gávea, Rio de Janeiro, Brazil, CEP 22451-100. Phone and fax: (+55-21) 2259-5046. Email: nsabrosa@terra.com.br.
Dr. Wong is a retinal specialist in London at Moorfields Eye Hospital and the Royal Free Hospital. He was previously a surgical retina fellow at Moorfields, an international pediatric retina research fellow at William Beaumont Hospital, and most recently a pediatric surgical retina fellow at Children’s Hospital Los Angeles. Email: chien22@yahoo.com.
1. Heimann H, Bartz-Schmidt KU, Bornfeld N, et al. Scleral Buckling versus Primary Vitrectomy in Rhegmatogenous Retinal Detachment Study Group. Scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment: A prospective randomized multicenter clinical study. Ophthalmology 2007;114:2142-2154.
2. SPR Study Group. View 2: The case for primary vitrectomy. Br J Ophthalmol 2003;87:784-787.
3. Shunmugam M, Shah AN, Hysi PG, Williamson TH. The pattern and distribution of retinal breaks in eyes with rhegmatogenous retinal detachment. Am J Ophthalmol 2014;157:221-226.
4. Schepens CL, Okamura ID, Brockhurst RJ. The scleral buckling procedures. Surgical techniques and management. AMA Arch Ophthalmol 1957;58(6):797-811.
5. Custodis E. Treatment of retinal detachment by circumscribed diathermal coagulation and by scleral depression in the area of tear caused by imbedding of a plastic implant. Klin Monbl Augenheilkd Augenarztl Fortbild 1956;129(4):476-495.
6. Lincoff HA, Baras I, Mclean J. Modifications to the Custodis procedure for Retinal Detachment. Arch Ophthalmol 1965;73:160-163.
7. Brazitikos PD, Androudi S, Christen WG, Stangos NT. Primary pars plana vitrectomy versus scleral buckle surgery for the treatment of pseudophakic retinal detachment: A randomized clinical trial. Retina 2005;25:957-964.
8. Schwartz SG, Kuhl DP, McPherson AR, et al. Twenty-year follow-up for scleral buckling. Arch Ophthalmol 2002;120 325-329.
9. Adelman RA, Parnes AJ, Sipperley JO, Ducournau D; European Vitreo-Retinal Society (EVRS) Retinal Detachment Study Group. Strategy for the management of complex retinal detachments: The European vitreo-retinal society retinal detachment study report 2. Ophthalmology 2013;120: 1809-1813.
10. Conart JB, Hubert I, Casillas M, Berrod JP. Results of scleral buckling for rhegmatogenous retinal detachment in phakic eyes. J Fr Ophtalmol 2013;36(3):255-260.
11. Ahmadieh H, Moradian S, Faghihi H, et al. Anatomic and visual outcomes of scleral buckling versus primary vitrectomy in pseudophakic and aphakic retinal detachment. Six-month follow-up results of a single operation—report number 1. Ophthalmology 2005;112:1421.
12. Vote BJ, Casswell AG. Retinal dialysis: Are we missing diagnostic opportunities? Eye 2004;18(7):709-713.
13. Wolfensberger TJ. Foveal reattachment after macula-off retinal detachment occurs faster after vitrectomy than after buckle surgery. Ophthalmology 2004;111:1340-1343.
14. Wilkinson CP. Visual results following scleral buckling for retinal detachments sparing the macula. Retina 1981;1:113-116.
15. McLeod D. Is it time to call time on the scleral buckle? Br J Ophthalmol 2004;88:1357-1359.
16. Mehta S, Blinder KJ, Shah GK, Grand MG. Pars plana vitrectomy versus combined pars plana vitrectomy and scleral buckle for primary repair of rhegmatogenous retinal detachment. Can J Ophthalmol 2011;46: 237-241.
17. Weichel ED, Martidis A, Fineman MS, McNamara JA, et al. Pars plana vitrectomy versus combined pars plana vitrectomy-scleral buckle for primary repair of pseudophakic retinal detachment. Ophthalmology 2006;113:2033-2040.
18. Leaver PK. Trends in vitreoretinal surgery—time to stop and think. Br J Ophthalmol 1999;83:385-386.
19. Feltgen N, Weiss C, Wolf S, et al. Scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment study (SPR Study): Recruitment list evaluation. Study report no. 2. Graefe’s Arch Clin Exp Ophthalmol 2007;245:803-809.
20. Mitry D, Awan MA, Borooah S, et al. Surgical outcome and risk stratification for primary retinal detachment repair: Results from the Scottish Retinal Detachment study. Br J Ophthalmol 2012;96:730-734.
21. Arya AV, Emerson JW, Engelbert M, et al. Surgical management of pseudophakic retinal detachments: a meta-analysis. Ophthalmology 2006;113:1724-1733.
22. Adelman RA, Parnes AJ, Sipperley JO, Ducournau D; European Vitreo-Retinal Society (EVRS) Retinal Detachment Study Group. Strategy for the management of complex retinal detachments: The European vitreo-retinal society retinal detachment study report 2. Ophthalmology 2013;120:1809-1813.
23. Tsui I. Scleral Buckle Removal: Indications and Outcomes. Surv Ophthalmol 2012;57:253-263.
24. Lorenzano D, Calabrese A, Fiormonte F. Extrusion and infection incidence in scleral buckling surgery with the use of silicone sponge: To soak or not to soak? An 11-year retrospective analysis. Eur J Ophthalmol 2007;17:399-403.
25. Heussen N, Hilgers RD, Heimann H, et al. for the SPR study Group. Scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment study (SPR Study): Multiple-event analysis of risk factors for reoperations. SPR Study report no. 4. Acta Ophthalmol 2011;89: 622-628.
26. Jackson TL, Donachie PH, Sallam A, Sparrow JM, Johnston RL. United Kingdom national ophthalmology database study of vitreoretinal surgery: Report 3, retinal detachment. Ophthalmology 2014;121:643-648.


