In the past few years, this trend toward minimizing tissue replacement has continued with the development of Descemet’s membrane endothelial keratoplasty, or DMEK, which replaces only the endothelial layer—the graft includes no stromal tissue. Results have been impressive, but the difficulty of the procedure has caused many surgeons to balk at attempting it. Here, four surgeons with extensive experience in corneal transplants share their thoughts on the current state of DMEK, and whether it’s reached the point at which it should be considered the procedure of choice.
How Good Is It?
“DMEK is ready for prime time, with certain caveats,” says Francis W. Price Jr., MD, president of the Price Vision Group in Indianapolis and founder and board president of the Cornea Research Foundation of America. (Dr. Price has done more than 1,000 DMEK procedures.) “DMEK is significantly better than any other transplant procedure. Postoperative visual acuity is better with DMEK; the wound sizes are smaller because we’re putting in less tissue; and the visual recovery is predictable—not as predictable as phaco, but pretty predictable. For that reason, when patients need to have both eyes done, we’re now beginning to do the eyes a week apart. The patients are doing really well. There are a few exceptions, of course; we have a few primary failures and some patients have residual edema. But for about 80 percent of these patients, we can do their eyes one week apart.
|
Mark A. Greiner, MD, assistant professor of cornea and external diseases at the University of Iowa hospitals and clinics and the Department of Ophthalmology and Visual Sciences, and assistant medical director at the Iowa Lions Eye Bank, has been doing DMEK, including fellowship training, since the spring of 2012. “I started on faculty at the University of Iowa that September, recommending the increased use of DMEK,” he says. “Since then, we’ve done about 150 cases in two years. I typically perform five to 10 DMEK cases a month.
“We’ve been impressed with our clinical results,” he continues. “I can get most patients into glasses a month after DMEK, where it takes six to eight weeks with DSAEK. And patients who have had DSAEK in one eye and DMEK in the other have remarked on their perceived improved visual benefits from DMEK. Even when the Snellen acuity is the same, patients almost invariably tell me that the DMEK eye has better vision. My interpretation is that without the stroma/stroma interface you have in DSAEK, you get less light scatter and thus have fewer higher-order aberrations.”
Mark A. Terry, MD, director of corneal services at the Devers Eye Institute in Portland, Ore., and professor of clinical ophthalmology at Oregon Health & Science University has been doing DMEK for about four years. “We now do about seven per week, 28 each month,” he says. “In comparing DMEK to DSAEK, we find that the quality of vision and the rapidity of visual improvement is better with DMEK.
|
The Learning Curve
In terms of the caveats to DMEK’s readiness for prime time, Dr. Price says the learning curve is a concern. (Difficulty mastering the procedure has clearly been a factor in many surgeons’ reluctance to undertake the procedure.) “DMEK is definitely more difficult to do than DSEK,” he notes. “The problem is, DMEK is just like phaco in that it takes a lot of pattern recognition and a lot of experience to do it well. If a surgeon had to start learning phaco from scratch instead of from a residency program, and he was only doing one or two phacos a month, he’d never get there. Maybe a few surgeons could master DMEK under those conditions, but the vast majority of surgeons could never accumulate enough experience to develop the necessary pattern recognition, the ability to intuitively know what’s going on in the surgery. Unfortunately, the only way to get that kind of extensive training is to do a fellowship at a center like ours, where multiple DMEKs are done each week.”
Dr. Terry notes that despite the complexity of DMEK surgery, it becomes routine once the surgeon has really learned to do it. “The key with DMEK is patience,” he says. “It’s not like DSAEK, where if you do the same thing over and over, you get the same result over and over again. With DMEK you have to recognize that one technique of unscrolling may be perfect for one piece of tissue and not work as well with the next graft. That’s why it’s important to have a repertoire of techniques and strategies to fall back on.” He adds that the need for patience extends to the tissue unscrolling. “One tissue may unscroll in a few seconds, while another might take nine or 10 minutes,” he says.
To help other surgeons learn DMEK, Dr. Price recently completed an electronic book on the topic with coauthor Yuri McKee, MD, titled The Digital Manual of Ophthalmic Surgery and Theory: DMEK. The iBook is available at the iTunes book section for $19.99, although the authors sometimes offer the book at a sale price of 99 cents (which they are doing in conjunction with this article for a three week period in September, 2014). “The reason we used the iBook format is that you can have unlimited photos, figures and video embedded into the text,” he explains. “So it’s like a textbook, but with all those additions. However, you can only download it onto an iPad or Mac with the Mavericks operating system.”
Given the learning curve problem, should a surgeon even attempt to add DMEK to his armamentarium if he has very few patients likely to need the surgery? “That’s highly surgeon-dependent,” says Dr. Terry. “ Some surgeons can do one or two DMEKs a month and be very good at it. Others will have a miserable time reaching and maintaining the necessary skill level with only one or two cases a month. Only the surgeon can make that decision. But if you want to offer DMEK, you have to commit to going through the learning curve. Then see how it goes; if you don’t start to feel comfortable with it after 10 cases, you have to decide whether that’s likely to change or whether you should stop and refer those patients to another surgeon from now on.”
The Argument for Waiting
Although everyone seems to agree that DMEK can produce better outcomes than DSEK, many surgeons feel that the potential benefits do not outweigh the drawbacks of the high learning curve. “DMEK is a wonderful procedure,” says William W. Culbertson, MD, director of the Bascom Palmer Eye Institute Laser Vision Center and professor of ophthalmology at the University of Miami Miller School of Medicine. “People get their improved vision earlier, and ultimately, they probably get a little bit better vision than patients with DSEK do. However, there are a number of practical problems standing in the way of its acceptance. If a surgeon could just do DMEK and have it be successful every time, it would be the procedure of choice. The problem is, right now DSEK has a higher success rate.”
| ||||||||||||




“Another problem is the logistics of having to redo your work if the graft doesn’t stick,” he says. “This may be easy to manage if DMEK is almost the only thing the surgeon does and he’s working in his own center, where he can just walk across the hall and try to reattach a graft with more air or more manipulation. But if you have to schedule this in a surgery center on a day that’s not your regular day, or do it after hours, and it can’t be easily done in the office or adjacent to the office, it becomes a logistical problem. It can also become a financial problem, because the patient’s insurance may not pay for a reoperation.
“Having to bring the patient back to rebubble the graft can have other consequences as well,” he notes. “In Florida, if you take a patient back to surgery within 30 days of the original surgery, it’s reportable to the state board. What happens next depends on how they interpret that. As surgeons, we all accept that DMEK is a worthwhile reason to take somebody back for reoperation, but it may not appear that way to the state board or insurance company. So you end up having to defend yourself to regulatory agencies and hospitals and boards.”
Dr. Culbertson also points out that DSEK has become very dependable, and patients are thrilled with its results. “I have yet to see a successful DSEK patient who wasn’t ecstatic,” he says. “Patients that have these surgeries go from 20/200 to 20/30 with DSEK, or from 20/200 to 20/20 with DMEK; they’re happy either way. So in terms of patient satisfaction, DSEK is every bit as good as DMEK.”
Dr. Culbertson says he doesn’t mean to be negative about DMEK. “I think it’s a wonderful operation,” he says. “When it gets more refined and dependable I think it will be the way to go.”
Settling on the Technique
Lack of a gold-standard technique for performing DMEK has been another factor leading surgeons to feel that the procedure might not be ready for prime time. Clearly, determining the most efficacious techniques is something that happens gradually over time as more and more surgeons perform the surgery. Today, an increasing number of surgeons are performing DMEK regularly; as a result, the surgery is gradually becoming safer, simpler and more successful. Many DMEK surgeons now believe a set of gold standard techniques is close to becoming a reality. Dr. Greiner says that from the surgeon’s perspective the main concerns are tissue preparation; tissue insertion; making sure that the tissue is oriented properly; and managing the complication of graft detachment, should it occur.
Regarding the tissue preparation, many surgeons worry about whether they should attempt to prepare the grafts themselves. Dr. Price notes that there are multiple concerns that might influence a surgeon’s choice—some technical and some practical. He points out that techniques for preparing the tissue in your own practice have now been refined to the point of having 1 percent tissue loss or less, as is the case at his practice. “That minimal loss rate has been replicated, not just using our technique but several others as well,” he says. “Friedrich E. Kruse, MD, in Germany has that level of preparation success, and eye banks are getting close to that. You can have an eye bank do the tissue preparation for you, but you’re going to be charged about $1,000 more for the extra processing. So which way you choose to proceed may depend on how you’re reimbursed, or if your facility cares about that charge.
“Of course, a lot of transplants are currently done by surgeons who don’t do very many,” he continues. “One result is that facilities may not even notice if they don’t get reimbursed. Sightlife, one of the largest eye banks, located in Seattle, looked at a lot of data from the Centers for Medicare & Medicaid Services and found that hospitals are often not paid for the tissue. Apparently, nobody complains, presumably because they don’t do very many grafts. We do more than 600 per year, so if we don’t get reimbursed for the cost of the tissue it’s a big deal. As a result, I’m always making sure we get paid. If we’re not getting paid I talk to the carriers or insurance companies and find out what’s going on.”
Dr. Greiner and his colleagues have worked closely with their eye bank partners at the Iowa Lions Eye Bank to refine the protocol for preparing DMEK grafts. “They do an excellent job of making prestripped and prepunched tissue available,” he says. “When we get the tissue in the OR, it’s already been prestripped from the host stroma and laid back down in its native anatomical position. In addition, surgeons can request that their DMEK tissue be subsequently punched with a trephine to their desired size; I like my tissue to be 7.5 mm in diameter.”
Finding the Best Injector
Another issue that has worried surgeons considering whether DMEK is ready for prime time has been settling on the best way to get the extremely fragile tissue into the anterior chamber. Today, the options appear to have been narrowed down to a few favorites, among which the leading DMEK surgeons seem split.
Dr. Price notes that getting a DMEK graft into the anterior chamber is totally different from injecting an IOL. “There are many different ways to put the graft in,” he observes. “Dr. Kruse in Germany and the surgeons at our center like to use IOL injectors—which is off-label, of course. I like that approach because it’s a totally closed system, although you have to choose an appropriate injector system. Only certain cartridges work. With the cartridge we prefer to use, we put the tissue into the cartridge and the plunger comes up behind it. It seals with the tip of the cartridge so that when you put it in the eye, you don’t have to worry about flow going back and forth.” Dr. Price says he prefers not to specify the injector they use, since it’s off-label, but surgeons interested in performing DMEK are welcome to ask him about it.
Dr. Greiner says when he was first starting to do DMEK he ran into trouble because the tissue insertion device was suboptimal. “I was using a Microstaar injector designed for IOL insertion with a foam plunger at the end,” he explains. “I was filling the back of the injector with a cohesive viscoelastic to get the graft to move out of the cartridge. Because it was an open system, when you advanced the plunger you could have egress of fluid or viscoelastic around the plunger or through the back of the cartridge. You couldn’t propel the tissue forward in a controlled way, and you had to use a viscoelastic agent.
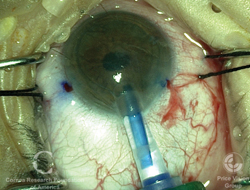
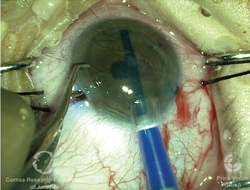
“We’ve switched to the off-label use of a Jones tube,” he continues. “This has allowed us to achieve control of the anterior chamber during tissue injection because it’s a closed system, which is incredibly important for the fluidics and tissue delivery during DMEK. The Jones tube we use can be coupled to a syringe filled with BSS, so we can eliminate the use of viscoelastic. In addition, the glass material is smoother on the inside than the plastic, and it doesn’t have as much electrostatic charge as the plastic does. As a result, we get a very smooth delivery.”
Dr. Terry, who uses the same glass tube as Dr. Greiner, notes that it was modified by his colleague Michael D. Straiko, MD. “He had the manufacturer change the shape so it would work with DMEK surgery,” he says. “A standard Jones tube is a straight glass tube that’s used for lacrimal surgery. But when you aspirate tissue into a straight injector, any suction pressure you apply to the other end of the injector will aspirate the tissue very quickly into the syringe. It makes the process hard to control. Dr. Straiko’s glass injector has a beveled tip, and it quickly balloons out into a wider tube. This modified tube is attached to a syringe by a coupling section made of standard plastic tubing. Now, when you draw back on the syringe the tissue is pulled into the outpouching area and stabilizes there. The tissue is far less likely to be damaged and the injection process is far smoother.”
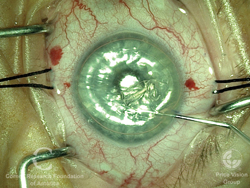
“In the Petri dish, the graft is scrolled up like a cigar,” says Dr. Greiner, adding that the tissue always scrolls with the endothelium on the outside. He notes that the glass tube is tapered to fit into a reasonably sized clear corneal incision. “I use a 2.8-mm keratome and enlarge the wound slightly to accommodate the tip of the glass tube,” he says.
Getting the Graft to Stick
Another concern that has discouraged surgeons from making DMEK a part of their armamentarium has been the tendency for the grafts to dislocate—an especially common problem during a surgeon’s learning curve. Dr. Greiner reports that significant progress has been made here as well.
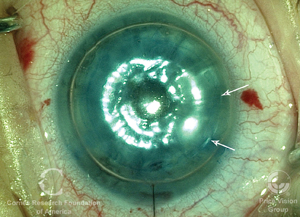
“Once the graft is centered, an air bubble is commonly used to hold the graft in place,” he explains. “The bubble presses the graft up against the stroma when the patient is lying on his back, nose to the ceiling. It helps the graft stay physically apposed to the host stroma and begin to self-adhere as the pump function in the graft tissue is waking up. The longer the bubble takes to go away, the longer the assisted apposition time.
“The biggest problem reported during DMEK surgeons’ learning curve is dislocation of the graft,” he continues. “Typically, this starts with lifting of the edges. Edge lifts can lead to progressive delamination of the graft and require a repeat injection of an air bubble. That certainly frustrated me when I first started doing DMEK surgery.
| ||||||
Dr. Greiner says he makes sure the anterior chamber is inflated with a bubble of SF6 20% for about 10 minutes to let the graft begin to adhere, although some of his colleagues give it 15 minutes. “After the waiting period we do an air-fluid exchange,” he says. “We make sure enough of the air bubble is removed to ensure that there is no air or gas trapped behind the iris, to minimize the chance of pupillary block. Once we’re sure no gas is trapped behind the iris, I reinflate with more gas, filling 80 to 90 percent of the anterior chamber.”
Still More Refinements
Dr. Greiner lists additional strategies that have been developed that are making DMEK more surgeon-friendly and helping to maximize the procedure’s success rate:
• If your grafts come from an eye bank, consider having the tissue stamped for ease of orientation. Especially for surgeons first attempting DMEK, determining whether the graft is right-side-up can be challenging. Dr. Greiner points out that some eye banks are now placing an S-stamp on the Descemet’s side of the graft. “This may be helpful if you’re just starting to do DMEK, or in cases with a challenging view of the eye,” he says.
• Perform an inferior peripheral iridotomy. “This will help minimize the chance of pupillary block from having air or gas trapped behind the iris,” explains Dr. Greiner. “I perform an inferior peripheral iridotomy intraoperatively, or in phakic cases, preoperatively with a laser.”
• Make sure the pupil can dilate and constrict as needed at different points during the surgery. “You want the pupil to do what you want it to do, when you want it to do it,” Dr. Greiner points out. “In order to facilitate the safe and successful unscrolling of the graft, you want a very constricted pupil. To achieve that, we use miochol, a short-acting miotic. Then, in order to minimize the complications associated with having an air or gas bubble inside the eye, you want the iris to dilate. So we typically avoid using strong, long-lasting miotic agents such as pilocarpine and miostat, precisely because we want to be able to modulate the pupil.
“I tend to apply my dilating eye drops after the tissue is unscrolled and centered, right before I float the graft with the air-gas bubble,” he adds. “That’s to make sure the dilating drops we use, cyclopentolate 1% and phenylephrine 2.5%, penetrate into the eye effectively. Once an air bubble is in there, it’s difficult for the topical drops to diffuse and produce appropriate dilation by the end of the case. So applying them before inserting the air bubble works best.”
• Consider using a retrobulbar block. “I know that many surgeons want to, and do, use topical anesthesia for DMEK, and that’s great,” says Dr. Greiner. “However, it’s very difficult for surgeons who are just making the leap from DSAEK to DMEK to feel comfortable knowing their patients are awake and moving while they may be struggling and less sure of themselves than they will be later on. Here at the University of Iowa, we use retrobulbar blocks for all of our DMEK patients. The retrobulbar block also causes pupillary dilation. That’s another reason to use a short-acting agent such as miochol to constrict the pupil before you inject the graft.”
• Learn multiple techniques for unscrolling the graft. Dr. Price notes that there are many ways to get the donor tissue to unfold. “We use different techniques with different eyes,” he says. “There are a variety of techniques that work.”
|

Dr. Terry notes that even if you choose this approach, it’s important to have multiple tapping maneuvers in your repertoire. “We call those manipulations ‘dance steps,’ because you’re dancing with the tissue,” he says. “We teach five dance steps in our DMEK course. For example, you may tap on the side of the cornea, or compress the peripheral cornea, or use two instruments to tap on the surface. With any given piece of tissue one dance step may work; with another tissue that manipulation may not work. Each tissue is a different thickness and different compliance, and may differ in how tightly it’s scrolled and how it unscrolls. By having five dance steps to choose from, you’ll have at least one strategy that will work for any given piece of tissue.”
Some surgeons, including Dr. Price, sometimes insert an air bubble inside the scrolled tissue to help it unscroll. Dr. Terry says his group doesn’t advocate that strategy. “We don’t feel it’s necessary if you use the dance steps,” he explains. “I know that Dr. Kruse puts an air bubble inside the scroll when the tissue is inside the injector, and that has worked extremely well for him. But that is technically a very difficult maneuver, so we don’t teach that option to beginning DMEK surgeons.”
What the Future Holds
Of course, whether or not a procedure is already considered ready for prime time, improvements will continue to appear. Dr. Price notes that there are still many ways DMEK can be improved. “Sometimes the donor grafts are nonfunctional,” he says. “We haven’t figured out why we get some of these primary failures; there’s no surgical problem to explain them. And we can always come up with better techniques, such as improving the way we put the tissue into the eye or finding an approach that will ensure that the graft always sticks. Another issue is that there’s sometimes a significant mismatch between the shape of the donor cornea and the patient’s cornea—which also sometimes happens in DSEK. This may degrade vision or make it harder for the graft to stick. At this point we don’t measure or match curvature, and most people do fine anyway, but it’s another factor that may eventually be improved. We’re working on all of these issues.”
Dr. Price believes that as more surgeons perform DMEK, the procedure will continue to improve. “More surgeons doing DMEK means different eyes looking at it and different thought processes,” he says. “Each person adds a little bit to the general knowledge. We saw that with DSEK; as more surgeons did it, the procedure got better and better. We’re going to see the same thing with DMEK.”
Dr. Culbertson agrees that DMEK is improving. “There have been step-by-step improvements in the technique,” he says. “DSEK started off the same way, with glitches and problems and rebubbling. But as more and more has been learned about it and the technique has been refined, it’s gotten to be much more dependable. I expect the same thing will happen with DMEK; and as dependability and technique improve, there will be greater acceptance of it.”
Drs. Greiner and Price agree, however, that DMEK is unlikely to ever totally replace DSEK. “Principally, that’s because not every patient has normal, straightforward anatomy,” says Dr. Greiner. “DMEK is my workhorse for normal anatomy, which most patients have. But I continue to use DSAEK for eyes with abnormal intraocular anatomy, or hardware in the eye from a previous surgery, such as a glaucoma drainage device, or a trabeculectomy, a large peripheral iridectomy or a core vitrectomy. These sorts of conditions can make it very difficult to execute successful DMEK surgery.”
So: Is It Ready?
Dr. Terry believes DMEK is ready for prime time. “If we didn’t believe that, we wouldn’t be teaching our courses,” he says. “I think patients should have the best procedure possible. Every surgeon should treat every patient as if he or she were a family member.
|
Dr. Greiner notes that all of DMEK’s surgical details are very nuanced. “It takes a lot of attention to detail to make sure you get a successful outcome,” he says. “Nevertheless, I believe this is the surgery to do in cases with straightforward intraocular anatomy. In our group, DMEK is the go-to procedure in cases of straightforward Fuchs’ endothelial dystrophy and pseudophakic bullous keratopathy. From our perspective, there’s no question—the potential for any downside is worth taking on the calculated risk. The advantages occur far more frequently, and are celebrated by both patients and surgeons.”
Dr. Culbertson says that whether DMEK is ready for prime time probably depends on the surgeon’s situation. “Some surgeons do a lot of DMEKs and have a setup that makes it easy to manage,” he says. “They get very experienced at it and have a high success rate, and it doesn’t interfere with the care of other patients in their office. But many surgeons aren’t in that situation. So when I weigh the two-line difference in outcomes against the hassle and expense of possibly having to take the patient back for additional procedures at addition cost and inconvenience, I come down in favor of DSEK. Again, I’ve never seen an unhappy DSEK patient, unless the patient had to have the procedure repeated. My goal is to make patients happy with the least inconvenience.”
In any case, Dr. Terry believes the question of whether DMEK is ready for prime time will soon be an obsolete issue. “In a few years we may still rely on DSAEK for complex cases such as anterior chamber IOLs and tubes,” he says, “but I think everyone will be doing DMEK for routine cases.”
Dr. Price adds that the challenges inherent in performing DMEK surgery are part of what makes being a surgeon enjoyable. “Most people who choose to be surgeons are going for a little gusto,” he says. “They get bored doing the same thing. Well, if you want to have adventure and challenges and an exciting time in the OR, DMEK is the procedure for you.” REVIEW
Dr. Price has a financial interest in the iBook on DMEK that he co-authored. Drs. Terry, Greiner and Culbertson have no financial interest in any item mentioned.
1. Coster DJ, Lowe MT, Keane MC, Williams KA; Australian Corneal Graft Registry Contributors. A comparison of lamellar and penetrating keratoplasty outcomes: a registry study. Ophthalmology 2014;121:5:979-87. doi: 10.1016/j.ophtha.2013.12.017. Epub 2014 Feb 1.
2. Yoeruek E, Bayyoud T, Hofmann J, Bartz-Schmidt KU. Novel maneuver facilitating Descemet membrane unfolding in the anterior chamber. Cornea 2013;32:3:370-3. doi: 10.1097/ICO.0b013e318254fa06.




