|
A broad lab workup was initiated, which included a complete blood count (CBC), comprehensive metabolic panel, anti-nuclear antibody (ANA), angiotensin converting enzyme (ACE), RPR, ESR, Lyme antibody titer, chest X-ray and HIV antibodies. MRI of the brain was done and was normal. The initial CBC was remarkable for leukopenia with a decreased white blood cell count at 2,900 cell/µL and anemia with a hemoglobin of 10.9 g/dL. Basic metabolic panel, ANA, ACE, RPR and chest X-ray were all within normal limits. ESR and liver function tests were found to be elevated. On day three of admission, his HIV test was found to be positive, with a CD4 count of 67 and a viral load of 77,800 copies/mL. A clinical diagnosis of progressive outer retinal necrosis was made. On day four, a repeat anterior chamber tap and intravitreal injection was performed.
|
Discussion
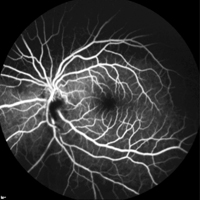
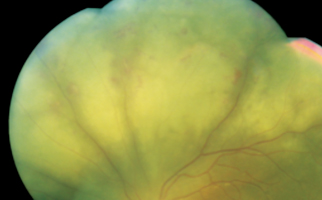
Progressive outer retinal necrosis (PORN), first described in 1990, is seen in patients who are immunocompromised (e.g., AIDS) who present with rapid outer retinal necrosis.1 Multifocal lesions with deep retinal opacification are characteristic of PORN. The lesions can be located in the peripheral retina with or without macular involvement. About 30 percent of patients have deep outer retinal lesions in the macula, which become confluent to form a cherry red spot. They classically have a “cracked mud” appearance where there is perivenular clearing of the retinal opacification (See Figure 4). There is minimal to no vasculitis. PORN differs from acute retinal necrosis syndrome in that there is minimal intraocular inflammation in PORN. The majority of patients have a poor visual outcome.2,3
|

CMV is a less common cause of progressive outer retinal necrosis, although there are a number of case reports of CMV PORN in the ophthalmologic literature. A report in 2002 described a 37-year-old Indian male with a clinical diagnosis of PORN who had a CMV-positive PCR, with negative PCR for HSV and VZV.5
While in the hospital, our patient was started on HAART therapy (emtricitabine/tenofovir and raltegravir) and double strength sulfamethoxazole and trimethoprim. He was monitored and on discharge, day 14, his final vision was stable at 20/80 (See Figure 5). Unfortunately, despite multiple attempts by both the Infectious Disease Department and the Wills Eye Retina Service to contact the patient, he did not return for further follow-up visits. REVIEW
The author would like to thank William E. Benson, MD, FACS, of the Wills Eye Retina Service for his time and assistance in preparing this case.
1. Forster DJ, Dugel PU, Frangieh GT, et al. Rapidly progressive outer retinal necrosis in the acquired immunodeficiency syndrome. Am J Ophthalmol 1990;110:341-8.
2. Margolis TP, Lowder CY, Holland GN, et al. Varicella-zoster virus retinitis in patients with acquired immunodeficiency syndrome. Am J Ophthalmol 1991;112:119-31.
3. Holland, GN. The Progressive Outer Retinal Necrosis Syndrome. Int Ophthalmol 1994;18:163-5.
4. Scott I, Luu K, Davis J. Intravitreal Antivirals in the Management of Patients with Acquired Immunodeficiency Syndrome with Progressive Outer Retinal Necrosis. Arch Ophthalmol 2002;120:1219-22.
5. Biswas J, Choudhry S, Priya K, Gopal L. Detection of cytomegalovirus from vitreous humor in a patient with progressive outer retinal necrosis. Indian J Ophthalmol 2002;50:319-21.


