|
In March, the Food and Drug Administration approved a new line of three femtosecond lasers by Ziemer (Port, Switzerland), designed to give ophthalmologists a choice regarding the features they want in their device. The Femto LDV Z models range from a laser made primarily to create LASIK flaps to one that can do flaps plus a range of corneal procedures. Here’s a look at the different designs and their features.
The LDV Z Line
Ziemer’s new lasers start with flap making at the entry level, the Z2. This laser uses the company’s low-pulse-energy, high-repetition rate femtosecond laser to make flaps of various widths and thicknesses, programmable by the surgeon. Next is the Z4, which, among other functions, allows surgeons to change the angle of the vertical cut of the flap, a process the company calls Z cuts. “Z-LASIK Z cuts impart different edge architectures to the flap,” says company President and Chief Executive Officer Frank Ziemer. “You can create an edge angle of 90 or 60 degrees, for instance, or an inverted angle. Though there are surgeons who prefer traditional edge cut architectures, the ones who prefer to change the angle say it helps the flap seal better.” The Z4 also allows the surgeon to create corneal tunnels for intracorneal ring segments and pockets for presbyopic corneal inlays such as the AcuFocus KAMRA, which isn’t approved in the United States.
The most fully featured of the LDV Z models is the Z6, which can do the functions of the Z2 and Z4 and can also perform lamellar and penetrating keratoplasties. It will also be the jumping off point for femtosecond-assisted cataract surgery in the future. “When the electronic and optical components are ready, we’ll have an upgrade package to perform steps of the cataract procedure,” says Mr. Ziemer. Just as the Z6 can eventually be upgraded to perform cataract surgery when that function becomes available, both the Z2 and Z4 can be upgraded to any of the higher Z levels on-site at the surgeon’s office.
A Look at the Features
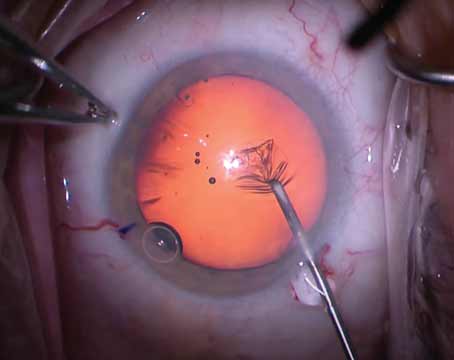
Scott MacRae, MD, director of the refractive surgery center at the University of Rochester’s Flaum Eye Institute, has used the Z6 for a small number of LASIK cases and one case of intracorneal ring segment implantation, and says he notices a difference between it and his previous Ziemer model. “The beds with the other laser were smooth, but the beds with this are very smooth,” he says. “I had two patients who saw 20/10 on the first day, which is pretty unusual.”
He also made use of the ablation customization options, and feels surgeons will appreciate those. “With the Z capacity, you can design any kind of edge that you want, and can put the hinge where you need it,” he says. “You can also create oval cuts. So, if you have a patient with a lot of astigmatism and want to create a little more space in the periphery, or if you have some blood vessels in a particular part of the cornea, you can use an oval cut for those situations.” He says the edge architecture customization can help the flap sit snugly like a manhole cover. “The more you minimize any gap or irregularity at the edge of the flap, the quicker the subjective recovery,” he says. “Patients are more comfortable and the optics are better.”
The Z4 and Z6 models that can create Intacs’ tunnels allow surgeons to create any variety of tunnel design they need. “You can design almost anything you could imagine from a geometric perspective,” says Mr. Ziemer, “as if you were drawing the tunnel on a piece of paper. You can change the tunnel’s arc length, the position, the width, depth and entrance cut. For the entry cut, it can be 90 degrees as you would make with a diamond knife or it can be a ramp of 60 or 30 degrees.”
|

Dr. MacRae says docking the device with the eye is straightforward. “Once you’ve applanated and have good suction, there’s one new feature that allows you to move the actual treatment in the x and y directions, and also allows you to rotate it,” he says. “For instance, you could rotate it to the exact spot you want the hinge to be after you’re applanated. This makes it easier because you don’t have to have it centered by way of centering the applanation only.”
Just to see the laser’s limits, the night before his first cases Dr. MacRae removed the epithelium from pig eyes and duped the system into creating 30-µm flaps. “The interesting thing was the cut was very smooth and there was no evidence that cavitation was going to break into the epithelium,” he says. “This tells me that, with a 90-µm flap, if the laser is calibrated correctly, you’re unlikely to have a bubble break through into the epithelium, which would essentially cause a buttonhole-type situation.”
Looking into the future, toward femtosecond cataract procedures, Dr. MacRae says Ziemer has to tackle the challenges that all femtosecond laser makers face. “Using optical coherence tomography, the farther you move back into the eye the more challenging it becomes to give an accurate diagnostic image,” he says. “This is a challenge because if you don’t have the distance correct in the OCT system of the laser, when you try to perform a nuclear fragmentation you can have torn posterior capsules. The other challenge is, even when you know what those distances are, you have to deliver the femtosecond laser to the right spot at that distance. Ziemer is able to have a small, tight energy bubble on the cornea, but the laser will have to go much deeper for the cataract procedure.”
He notes that the farther from the laser aperture it is the more elongated the laser beam will be in the vertical dimension, i.e., downward into the eye; this would be the challenge with any laser. “This doesn’t make much of a difference when you’re doing a capsulotomy,” says Dr. MacRae. “But having vertical elongation is bad when you’re trying to do nuclear dissection, because of the presence of the posterior capsule.”
Mr. Ziemer says the LDV Z series’ main benefit is upgradability, allowing surgeons to avoid adopting technology that ultimately leads to a dead end. “Once you have the Z6,” he says, “the machine is ready to be upgraded even more for cataract. The platform doesn’t come to an end when you have the Z6.” REVIEW