IOLMaster 700
With the IOLMaster 700, Carl Zeiss Meditec AG did more than update the popular IOLMaster 500: The newest iteration uses swept-source OCT to visualize the full length of the eye, enabling the detection of unusual ocular geometry and crystalline lens tilt to assist with predicting the effective lens position. “For the first time, the examiner really sees what he is measuring. Because the IOLMaster 700 is an OCT machine, one sees the fovea, the lens and the cornea,” notes Walter Sekundo, MD, PhD, professor and chairman, Department of Ophthalmology, Philipps University Hospital of Marburg in Germany.
 |
| Patient’s (top) and user’s (bottom) views of the IOLMaster 700, a swept-source OCT device. |
Zeiss claims that the new IOLMaster can penetrate 99 percent of cataracts. A study1 comparing AL, anterior chamber depth and K-value measurements obtained by the IOLMaster 700 and the IOLMaster 500 found that while the agreement between the two devices was excellent, only the IOLMaster 700 could measure through all 188 of the subject eyes. The same study indicated that when using formulae requiring white-to-white, there might be less agreement between the devices than with formulae that don’t require this variable.
At 2,000 scans per second, the IOLMaster 700 measures axial length, anterior chamber depth, central corneal thickness and lens thickness quickly. Users can gather comprehensive data easily, according to Dr. Sekundo, who values the IOLMaster 700’s simplicity. “Push the button once and you get everything you need,” he says.
Zeiss says that the new IOLMaster’s SS-OCT technology allows it to detect irregular eye geometry. One study showed that while it’s not a substitute for a dedicated retinal OCT scan, the IOLMaster 700 may help pick up macular pathologies, particularly intraretinal fluid and macular holes, in patients seen for pre-cataract surgery biometry.2
The IOLMaster 700 includes Zeiss’s “telecentric keratometry,” producing highly repeatable, distance-independent corneal surface measurements. New capabilities include CCT and LT measurements. The biometer’s Fixation Check feature alerts the user to a suboptimal scan if the resulting image doesn’t show the foveal pit. “The examiner can check the position of the reference points, and either confirm or reject the exam,” explains Dr. Sekundo, who adds, “With all laser interferometry biometry the examiner relies on the patient’s good fixation.”
For toric lens implantation, the IOLMaster 700 allows the surgeon to compare a reference image of the eye that uses blood vessels as landmarks to delineate the axis of the intraoperative eye. External marking is not necessary to achieve proper alignment. The device’s onboard formulae include the Haigis Suite (Haigis, Haigis-L for post-refractive surgery eyes, and Haigis-T for torics); Hoffer Q, Holladay 2 and SRK/T. The IOLMaster 700 also has a built-in toric calculator, eliminating the need to use a lens manufacturer’s calculator.
IOLMaster 700 users can continue to use the optimized IOL constants for more than 270 lenses from the User Group Laser Interface Biometry (ULIB) database.
Lenstar LS900
The Lenstar LS900 is an optical low-coherence reflectometry device. Manufacturer Haag-Streit says that the Lenstar, which made its debut in 2009, was the first optical biometer on the market able to measure crystalline lens thickness. The Lenstar LS900 also measures AL, corneal thickness, ACD, aqueous depth, corneal curvature, radii of the flat and steep meridians, axis of the flat meridian, WTW and pupil diameter.
For patient comfort, Lenstar’s Automated Positioning System tracks eye movement to capture reliable measurements in one click. The user can select Dense Cataract Mode, and can also select for aphakic, pseudophakic or silicone oil-filled eyes before or after completing a scan. “What I like about the Lenstar is the ease of use. It just takes one click of the button to get K readings, topography, anterior chamber depth, lens thickness and axial length,” says Edward Meier, MD, director of clinical research at Apex Eye in Cincinnati, Ohio.
A dual-zone keratometry measurement system with 32 closely spaced measurement points captures the spherical equivalent and axis. For extra assurance when planning for toric or premium IOLs, the Pro version of the Lenstar LS900 comes with the option to add the T-Cone, a double-ring (1.65-mm and 2.3-mm diameter) placido disk topographer that measures a 6-mm optical zone. Another option is the EyeSuite IOL toric planner software, which includes the Barrett Toric Calculator. “The corneal measurements are so accurate you don’t need to get separate K readings on another device for toric IOL planning,” says Dr. Meier. “The other part that I like is that the EyeSuite software automatically populates the newest lens calculation methods, including Hill RBF, Barrett and Olsen.”
The range of measurements that the Lenstar LS900 takes is required for modern IOL formulae. The Lenstar LS900 includes the following: Barrett Universal II; Barrett True-K; Haigis; HofferQ; Holladay 1; SRK/T; SRK II; Masket; Modified Masket; and Shammas No-history. In late 2016, the Lenstar LS900 also integrated the Hill RBF Method into its software, and previous adopters of the Lenstar LS900 received the update. The Hill RBF Method of IOL power prediction is based on machine learning using feature extraction and matching, and is designed to interpolate missing data and gain accuracy as it accrues experience. Holladay IOL Consultant Professional, Olsen and Okulix’s ray-tracing methods are available via an additional software interface. Dr. Meier says that the Hill RBF method is his go-to for lens power calculation. “For toric strength and axis, I use the Barrett toric formula,” he adds.
Dr. Meier says that the Lenstar LS900 simplifies toric IOL procedures. “I don’t need to use a different machine to measure K readings if I’m planning on a toric lens implant,” he says. The printout from EyeSuite gives me the lens power for as many formulae as I want to see. It also calculates toric lens power right on the printout. I can just look at the report and see if my patient would benefit from a toric implant, without having to calculate K’s in my head.”
Aladdin HW3.0
Topcon’s new combination biometer and corneal topographer obtained FDA clearance for U.S. distribution in late February 2017. Topcon says the Aladdin HW3.0, a low-coherence interferometry biometer and placido topographer, can get the measurements needed for refractive cataract surgery with the manufacturer’s goals of speed, accuracy and ease of use in mind.
For Jose A. Mendoza MD, MS, in practice at Oftalmo Salud-Lima, Lima, Peru, the device helps keep patient flow moving while ensuring the accuracy of his IOL power predictions. “All of the important biometric measurements, for example, lens thickness, central corneal thickness and anterior chamber depth, are derived from interferometry, instead of a split beam as was used in prior versions,” he says, adding that the new technology has aided IOL power calculation by more accurately predicting effective lens position.
Three-zone keratometry at 3, 5, and 7 mm from the central cornea measures K’s, and 24 placido rings map the cornea. The Aladdin’s dynamic pupillometry allows users to see lens centration and the contraction and dilation of the pupil under photopic and mesopic conditions to assist in premium IOL selection. Zernike wavefront analysis evaluates higher-order aberrations and corneal surface anomalies like early-stage keratoconus. “The fact that Aladdin comes with a corneal topographer and also wavefront analysis helps us to decide which patients would be suitable for premium IOL implantation,” says Dr. Mendoza.
The Aladdin biometer has demonstrated good agreement with the IOLMaster 500 in terms of AL, ACD and mean K-values.3
The Aladdin includes a built-in calculator that works with any commercially available toric IOL. The device’s software features SRK/T, Holladay 1, Haigis, and Shammas No-history and the Camellin-Calossi formula for post-refractive surgery eyes. The Barrett IOL Suite and the Abulafia-Koch Regression Formula for toric lens selection are integrated into the device. “The new formulas it includes, such as the Barrett formula, provide an intuitive platform for the calculation of the cylindrical power and the placement axis of toric IOLs in astigmatic patients,” says Dr. Mendoza. “The Toric IOL calculator and the simulation of the surgical outcome using this tool are really useful in our clinic, since we manage a lot of cataract patients with high astigmatism.”
After taking measurements, users can save or print out an IOL report that identifies the lens power predicted to give the best refractive outcome. The Aladdin HW3.0 also generates the Measurement Report, a summary of all the data gathered for both eyes, as well as an Aladdin Report that alerts the user to any findings that could even subtly influence the performance of a premium IOL.
Dr. Mendoza says that in his busy practice, most cataract patients don’t present for surgery until their cataracts are advanced; he reports the ability to scan through for axial length on about 30 percent more patients than before adopting the Aladdin HW3.0. “Since we started working with the new Aladdin, our surgical outcomes in hard-cataract patients are much better,” he says. “Ultrasound biometry still is, as many colleagues think, the gold standard, but it requires a very well-trained person to perform it and get reliable data. Taking all the measurements in one instrument with a single touch makes our workflow more efficient.”
AL-Scan
The AL-Scan measures axial length, anterior chamber depth, pupil size, WTW, central corneal thickness and keratometry in 10 seconds with ease, according to manufacturer Nidek. “The device is very easy to use, and technicians find it quick and very straightforward,” says Sheraz Daya, MD, FACP, FACS,
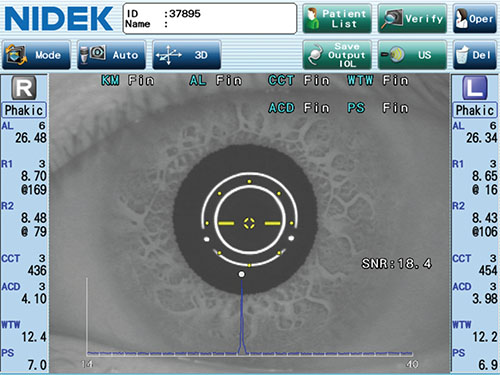 |
| The AL-Scan has an auto-tracking feature that follows patients’ eye movements along the X, Y and Z planes; auto-shot takes the scan at the moment of proper alignment. |
Nidek says that preop measurements are easy for the patient as well as the operator of the AL-Scan, thanks to the biometer’s 3D auto-tracking and auto-shot features: Auto-tracking follows the patient’s eye movements along the X, Y and Z planes, while auto-shot takes the scan as soon as it senses correct alignment, for valid data with minimal fuss. Auto-tracking and auto-shot can facilitate collecting trustworthy data even from restless patients. “Auto-tracking improves usability; the technicians just love this feature,” Dr. Daya notes.
Scheimpflug imaging captures CCT and ACD, which help to assess the depth of the cataract. Topography and keratometry with double mire rings reflected onto the cornea aid in evaluating for aberrations. The AL-Scan zeros in on optical landmarks in the eye to measure the angle from the steepest meridian. This axis determination aids the alignment of toric lenses.
Dr. Daya considers the AL-Scan a reliable source of multiple measurements using one device. “Three years ago we compared its performance to the IOLmaster 500 and found there was no difference in terms of measures and IOL calculations. It compared well to Pentacam keratometry. The device also has a built in ultrasound A-scan and a pachymeter,” he says.
Surgeons can use the AL-Scan’s constant-optimization feature to fine-tune IOL constants for results that can continually improve. The AL-Scan incorporates IOL formulae including Camellin-Calossi for post-refractive eyes; SRK/T, Shammas PL; Binkhorst, Regression; Regression II; HofferQ; Haigis and Holladay.
Nidek says that the AL-Scan has the ability to penetrate even dense cataracts by adjusting signal-to-noise ratio to amplify the signal, but the AL-Scan also offers an optional built-in ultrasound biometer to avoid moving patients to another machine if an A-scan is needed. “Although calculations can be performed with dense cataracts, there is the odd time when having the ultrasound device readily available is useful,” Dr. Daya notes.
Argos
Relative newcomer Argos (Movu) attained FDA clearance in 2015. It uses swept-source OCT to get whole-eye scanning in a single 0.6-second capture, according to the manufacturer. The Argos measures AL, CCT, aqueous depth, ACD, LT, pupil size, WTW, K’s and astigmatism.
Dense Cataract Mode allows the Argos to acquire data that other biometers may not get, according to Daniel Kim, MD, medical director of St. Mary’s Eye & Surgery Center, Palisades Park, N.J. “Axial length acquisition rate is high, even in dense cataracts,” he says. “There are fewer patients that need to be referred to A-scan.” He also appreciates the speed at which the measurements are captured, adding, “A fast acquisition rate means that repeatability is great, and the patient does not need to be fixated for as long as with other biometers.”
 |
| Manufacturer Movu says that the Argos acquires axial length, central corneal thickness, aqueous depth, anterior chamber depth, lens thickness, pupil size, white-to-white and keratometry quickly, making scans easy on patients. |
William B. Trattler, MD, Center for Excellence in Eye Care, Miami, Fla., also appreciates the Argos’ ability to measure eyes with advanced cataracts. “The Argos biometer has made a significant impact to our practice in that it has dramatically reduced our need to perform ultrasound biometry,” he says.
The Argos features an analysis mode that allows the surgeon to verify the results of collected measurements. “Analyze Mode allows our technicians to check the plausibility of the biometric values,” Dr. Kim explains. “Having the OCT image available confirms that the measured parameters do actually align with correct boundaries. There are also indicators if the patient was not fixated during measurement, or of any other complications that would not necessarily be detected by biometers that do not provide a whole image of the eye.”
The Argos’ IOL power formulae include the Barrett Suite, Hoffer Q, Haigis, Holladay I, SRK/T and Shammas No-history.
“We like that the Argos has the Barrett Universal II formula as well as the Barrett True K formula integrated,” says Dr. Trattler. “It also has a toric IOL calculator built in that can use these formulas, so we don’t need to export our data to web-based planning software,” he adds, noting that this helps avoid refractive surprises stemming from manual transcription errors.
Dr. Trattler says he combines data from the Argos with corneal mapping. “We typically use a placido disc topographer for evaluating the corneal shape, as well as the Cassini topography system, which we use for posterior corneal astigmatism measurements,” he says.
Pentacam AXL
In addition to the Argos, the Pentacam AXL from Oculus has a valued role in Dr. Trattler’s practice. “The Pentacam AXL is a very robust device that combines corneal imaging with axial length measurements,” he says. “Its strength is the software, which can provide an incredible level of information about the anterior segment of the eye. The tomography software provides corneal shape images and corneal shape analysis. The integrated software can be used to determine whether a patient is an appropriate candidate for LASIK, if it’s needed after cataract surgery,” he says.
The Pentacam AXL combines the Scheimpflug imaging of the original Pentacam with a PCI biometer. The Pentacam AXL takes a succession of AL measurements, and the software selects the best one to render a three-dimensional image of the anterior segment.
The Pentacam’s Scheimpflug camera technology allows it to assess corneal topography, taking into account irregularities and astigmatism of both the anterior and posterior corneal surfaces.
Another feature of the Pentacam AXL’s software is the ability to estimate changes in the corneal shape incurred by previous PRK or LASIK, based on its current evaluation of the shape of the cornea. “The Pentacam AXL can provide an approximation of the patient’s pre-LASIK level of myopia or hyperopia,” Dr. Trattler explains.
The Pentacam AXL’s combination of measurements, including CCT and WTW in addition to topography, keratometry and AL, are entered into the IOL calculation software automatically, so transcription errors aren’t a concern. The device will also measure the density of cataract and grade corneal opacities. “The Pentacam AXL can also evaluate the average angle depth, and is therefore useful for documenting and evaluating cases with narrow angle,” says Dr. Trattler. “Another important aspect of the device is its assessment of corneal thickness. This is useful in patients who have Fuchs’, so we can measure corneal thickness both before and after surgery to determine if the corneal thickness has returned to baseline postop.”
The CCT measurement is also important for modern IOL power calculation; the Pentacam AXL’s IOL power calculator includes formulae for normal eyes and post-refractive surgery eyes, among them Haigis, SRK/T, Holladay 1, Hoffer Q, Potvin-Shammas-Hill and Potvin-Hill. An integrated IOL database helps surgeons select the right lens at the correct power.
The Pentacam AXL generates multiple reports, including the Fast Scanning Report, which can alert the user to keratoconus and other corneal changes, as well as anterior chamber irregularities. The Pentacam AXL’s Belin/Ambrósio Enhanced Ectasia Display function can detect ectatic conditions such as posterior keratoconus or post-LASIK ectasia.
The ability to measure irregularities on both corneal surfaces and wavefront analysis capability assist with premium IOL planning. The operator simply focuses on the center of the patient’s pupil to get Oculus’ Total Corneal Power Map. The Total Corneal Power Map calculates corneal power based on anterior and posterior astigmatism, which can help in planning toric IOL implantations. REVIEW
Dr. Sekundo is a consultant for Carl Zeiss Meditec AG. Dr. Daya is a consultant for Nidek. Dr. Kim is a consultant for Santec USA Corporation, parent company of Movu. Dr. Trattler is a consultant for Santec USA Corporation and Oculus. Drs. Meier and Mendoza report no relevant financial disclosures.
1. Akman A, Asena L, Güngör SG. Evaluation and comparison of the new swept source OCT-based IOLMaster 700 with the IOLMaster 500.Br J Ophthalmol 2016;100:1201–1205.
2. Hirnschall N, Leisser C, Radda S, Maedel S, Findl O. Macular disease detection with a swept-source optical coherence tomography-based biometry device in patients scheduled for cataract surgery. J Cataract Refract Surg 2016;42:530-6.
3. Mandal P, Barrow EJ, Naroo SA, et al. Validity and repeatability of the Aladdin ocular biometer. Br J Ophthalmol 2014;98:256-8.
4. Shammas HJ, Ortiz S, Shammas MC, Kim SH, Chong C. Biometry measurements using a new large-coherence-length swept-source optical coherence tomographer. J Cataract Refract Surg 2016;42:50-61.


