While complications with phakic intraocular lenses are rare, they can still arise, according to John A. Vukich, MD, assistant clinical professor at the University of Wisconsin, Madison, and medical monitor for the Visian Intraocular Contact Lens (Visian ICL) U.S. clinical trials for STAAR Surgical, of Monrovia, Calif.
"The major complications of phakic IOLs are well-described by the two clinical trials held in the United States for the Verisyse and the Visian ICL. This provides the most comprehensive audited data as they were part of multicenter FDA trials," notes Dr. Vukich, who has performed 156 phakic IOL cases with the Visian ICL.
"Both lenses had a low complication rate. There was less than 1 percent in developing cataract. The rate was 0.6 percent for the Verisyse and 0.9 percent for the Visian," he explains.
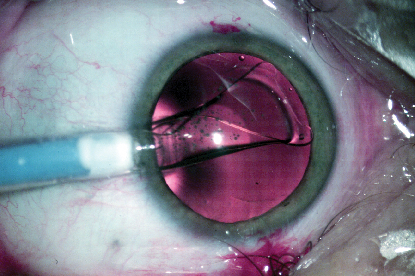 |
| The Visian ICL, from Staar Surgical. Phakic lenses approved in the United States have a complication rate of less than 1 percent in clinical trials. Photo: Stephen G. Slade, MD |
The Artisan/Verisyse phakic IOL, from Ophtec USA, of Boca Raton, Fla., was approved in September. Ophtec markets the product under the trade name Artisan, while Advanced Medical Optics (AMO), of Santa Ana, Calif., has global distribution rights and markets the product under the name Verisyse, which it has done in Europe since 2002. AMO is the exclusive distributor for the product in North America and Japan.
The Visian ICL is currently marketed in Europe. The Visian ICL myopic and toric U.S. trials are complete, while the hyperopic trial still has limited enrollment. In the United States, the Visian ICL is still pending final approval, although the FDA's Ophthalmic Devices Panel recommended approved it in October 2003.
Concerns and Complications
"There really weren't that many complications," Dr. Vukich says. "Elevation of intraocular pressure has not proven to be a problem, nor has retinal detachment. All of these patients are nearsighted and have baseline elevated risks over the normal population, so routine eye care is going to be an essential part ongoing eye care as well."
Other complications are rare, and relate primarily to known risks of intraocular surgery, he explains.
David R. Hardten, MD, director of refractive surgery at Minnesota Eye Consultants, notes that phakic IOLs yield excellent vision quality even in very high corrections. "There is less potential for irregular astigmatism at the very high corrections," he notes.
The potential for intraocular complications exists, says Dr. Hardten. Cataracts, endothelial problems and iris complications are uncommon, but could be more severe.
 |
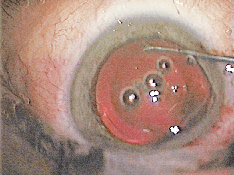 |
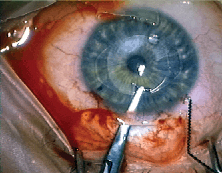
| Users suggest surgeons take care during initial cases involving the Artisan/Verisyse lens; the lens must be held in one hand while enclavating the haptic with the other. Photos: David R. Hardten, MD | |
"Although with careful surgical procedure and careful attention to learning the nuances of each IOL type insertion these will be less," he adds.
Now that phakics are becoming available to more surgeons, additional complications may arise in less experienced surgical hands. "Most likely, the main concern will be wound problems, such as wound leak," notes Dr. Hardten.
Richard L. Lindstrom, MD, founder and managing partner of Minnesota Eye Consultants, adds that in less experienced surgical hands, the same complications found in the clinical trial might arise at a higher frequency in the beginning. However, the learning curve in the study was about 10 cases, after which a precipitous fall in complication rate occurred, he says.
"All the same complications of intraocular surgery are possible at a similar but minimal rate, with cataract being higher and retinal detachment and cystoid macular edema being lower," he says.
In addition, lenses could need to be repositioned, removed or replaced, as would be expected for any implant, adds Dr. Vukich.
Hands-on Training
Copious training is critical. "We have a great deal of experience in training new physicians in the use of the Visian ICL, says Dr. Vukich, who notes that in a series of patients implanted by surgeons who are new to this technique the results closely mirrored those in multicenter U.S. trial. "The learning curve can be fairly short with proper proctoring and training," he adds.
In order to avoid complications, surgeons should be practiced and confident before they start. "Careful training should avoid most problems, although even with best efforts, complications can arise," says Dr. Hardten.
Dr. Hardten and his colleagues have implanted 20 ICL's and about 150 Verisyse implants in addition to many natural lens replacements with capsular bag implants. He notes that each has a use in different situations depending on the case.
Stephen G. Slade, MD, in private practice in Houston, Texas, and clinical investigator for the Staar ICL, says complications may be more likely at the beginning of a surgeon"s learning curve with a new procedure.
"In the initial learning curve, the surgeon may be more apt to see a cataract, more corneal edema, or have a temporary rise or elevation of pressure," says Dr. Slade, who now directs the courses that teach surgeons to perform the Visian ICL procedure along with Dr. Vukich.
Dr. Slade recommends that surgeons take the course that the manufacturer recommends and also spend time meeting with other surgeons who are experienced with phakic IOLs.
"Ideally, surgeons should have an experienced surgeon with them on their first cases to offer advice if needed," he says, noting that they should also follow their first cases especially closely.
Careful patient selection of a surgeon's first phakic cases is also key, says Dr. Slade. For example, select motivated, well-educated, patients with reasonable expectations. Also a patient with favorable anatomy, such as a deep anterior chamber and good exposure will help.
In addition, he recommends that surgeons keep up with the progress of the technology. "Surgeons should go to user group meetings, get on chat lines, and read new information as it is presented so that they are aware of all the advances. This is important because whenever a new technology is approved many good ideas usually come up in the first year or so as hundreds of surgeons start using the technology," Dr. Slade says.
Other Potential Issues
Blurry or cloudy vision may also be a concern. In terms of quality of vision problems, the most common problem will still be residual refractive error, just as in any refractive surgery, says Dr. Hardten. "Any other complication, such as wound problems, cataracts, etc., would result in blurred vision," he adds.
Dr. Vukich agrees that blurred vision is the end result of any number of problems. "With phakic IOLs, the most likely reason would be a miscalculation of selected implant power," he says. "Then a surface enhancement with laser or an exchange of lens may be indicated. We have not seen any instances of corneal decompensation as result of the use of this implant. Also, visually significant cataracts will cause cloudiness of vision. I do consider this an unusual event but it is still a possibility."
Concerns relating to endothelial cell loss were raised for both devices. "The endothelial cell count at this point has not been definitively proven to remain stable," says Dr. Vukich. "However, trend lines are encouraging and at this point preoperative determination of adequate endothelial cell density will be required in the labeling for both devices."
Dr. Hardten adds, "The potential for endothelial cell loss is also a concern anytime you do surgery in the eye. However, endothelial cell counts have been very stable in the studies to date. There is some early loss, and variable amounts of loss from study to study, but overall results look safe for the endothelium."
Pearls for Phakics
According to Robert K. Maloney, of Maloney Vision Center, for beginning surgeons with the Verisyse lens the most common complication will be touching or in some way damaging the endothelium because the lens has to be held in one hand and the haptic is enclavated with the other hand.
"If the surgeon is not careful and not paying attention the lens could be tilted up and ding the epithelium," says Dr. Maloney, a clinical investigator for Verisyse, who has performed approximately 100 cases.
Dr. Maloney pointed out that there are several steps surgeons can take to reduce the chance of complications with phakic implantation.
In the preop evaluation, surgeons want to be certain that the patient's anterior chamber is sufficiently deep, more than 3.2 mm, so there is enough room to implant the lens. "My experience is that all myopes have a deep enough AC, but often hyperopes do not," he says.
Surgeons also want to have careful patient selection be sure that the patient has a reasonably dense endothelial mosaic. "I avoid patients who have conditions that can cause inflammation of the AC, such as diabetes. However, I do not think that pigment dispersion is a contraindication, although we haven't treated anybody like that yet," Dr. Maloney says.
Intraoperatively, a good limbal incision is important (with the Artisan/Verisyse lens) because the posterior lip needs to be far enough anterior to prevent iris prolapse, Dr. Maloney explains.
| Possible Phakic IOL Complications |
| Cataract Decentration Endophthalmitis Endothelial problems Infections Iris complications Wound problems, i.e., wound leak Retinal detachment Cystoid macular edema Uveitis Temporary rise in IOP Lens repositioning or removal |
Sideport incisions also need to be carefully constructed with this lens. "Sideport incisions need to be the right distance apart and they need to be at the correct angle," he explains. "For example, cataract surgeons are used to making sideport incisions that are parallel to the iris and radial in direction. For the Verisyse lens, the sideport incisions are angled inferiorly rather than radially and angled posteriorly rather than remaining in the iris plane."
The most difficult part of the Verisyse procedure is the enclavation step. This is something, however, that most surgeons can master after five or 10 lenses, he adds.
Because these high myopes have a thick sclera, Dr. Maloney does not use a scleral incision. "I think they are more likely to leak," he says. "I prefer a limbal incision. One needs to make sure the incision is sufficiently tight so it won't leak. It takes surgeons back to the days when they weren't doing self-sealing sutureless cataract surgery. So surgeons have to pull out their needle holder and thread again."
Dr. Maloney positions the incision in the meridian to reduce any pre-existing astigmatism. Sutures are then removed three to four weeks postoperatively.
The Future
It's a very exciting time now in ophthalmology with phakic IOLs beginning to be approved in the United States. Dr. Lindstrom summarizes the major benefits of phakic IOLs as their usefulness for higher levels of myopia, high quality of vision with minimal induction of higher-order aberrations, a rapid visual recovery, and potential reversibility.
Dr. Hardten agrees. "With phakic IOLs, vision quality is excellent, even in very high corrections. There is less potential for irregular astigmatism at the very high corrections," he says.
For more information see "Phakic Intraocular Lenses: Principles and Practice," edited by Hardten, DR, Lindstrom, RL, and Davis, EA. Thoroughfare, NJ: Slack Publishing, 2004.