A 49-year-old Caucasian female was managed by a general ophthalmologist for intermittent pain and redness of her right eye. The patient had initially presented to the general ophthalmologist eight months prior, at which time it was noted that she had sectoral injection of her superficial and deep episceral blood vessels with a normal dilated fundus examination, suggestive of episcleritis or scleritis. She was advised to take oral naproxen, but there was minimal improvement of her signs and symptoms, despite compliance with her medication.
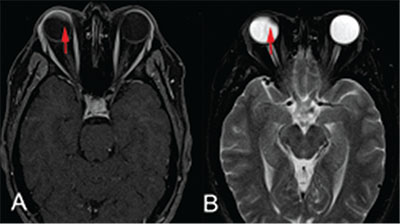 |
| Figure 1. Post-contrast (A) T1-weighted magnetic resonance imaging with fat suppression and gadolinium enhancement, and (B) T2-weighted magnetic resonance imaging of brain and orbits showing an intraocular mass in the right eye, as indicated by arrow. |
The ophthalmologist tried several other regimens over the next few months, including topical prednisolone acetate 1%, topical difluprednate 0.05%, topical olpatadine 0.2% and topical cyclosporine 0.05%. However, none of these medications helped to relieve her symptoms. Approximately one month prior to presentation, she developed a constant, severe headache, lasting more than five hours per day. Repeat dilated fundus examination at that time demonstrated a mass in her right eye, suspicious for ring melanoma despite best-corrected visual acuity of 20/20 in both eyes. As part of her workup, she had magnetic resonance imaging of her brain and orbits, which was concerning for an intraocular mass (Figure 1). Based on these findings, she was referred to Wills Eye Hospital’s ocular oncology service for further evaluation.
Medical History
 |
Examination
Ocular examination revealed best-corrected visual acuity of 20/20 in each eye. The pupils were equal, round and reactive bilaterally without afferent pupillary defect. Extraocular motility and confrontation visual field exam were full OU. Intraocular pressure by Goldmann applanation tonometry was 18 mmHg OD and 17 mmHg OS. Anterior segment and dilated fundus examination OS were unremarkable.
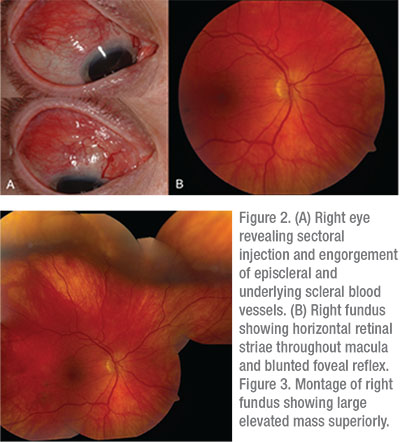
The anterior segment OD revealed sectoral injection of the superficial and deep episcleral blood vessels from 9 to 3 o’clock (Figure 2A). On dilated fundus examination the optic nerve and blood vessels were within normal limits, but there were horizontal retinal striae throughout the macula, a blunted foveal reflex and a large elevated mass measuring approximately 25 mm at its base and 5 mm in thickness and without subretinal fluid (Figures 2B and 3).
Please click this link for diagnosis, workup, treatment and discussion.


