A 25-year-old woman presented for emergent evaluation of severe pain, tearing and blurred vision in the right eye. She had been seen by an outside ophthalmologist one month prior and was diagnosed with a corneal ulcer. She was treated with moxifloxacin 0.5% every hour and trifluridine 1% nine times per day. Despite treatment, her symptoms progressed. She reported a history of soft contact lens wear; however, she denied wearing them in the months prior to presentation. There was no history of trauma to or foreign material in the eye. She reported hot tub use several months prior.
Medical History
The patient had an ocular history of corneal ulcer in the right eye four years prior to presentation which had resolved with topical antibiotics. She had no history of eye surgery. She had no other medical history and was not taking any other medications. She denied tobacco or alcohol use. A full review of systems was
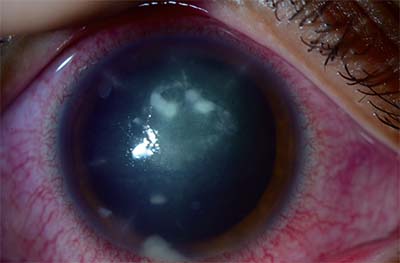 |
| Figure 1. Anterior segment photograph of the right eye on presentation showing a multifocal infiltrate with anterior chamber reaction and dense radial keratitis. |
Examination
Visual acuity with correction was count fingers at one meter in the right eye and 20/25 in the left. External examination showed mild edema and reactive ptosis of the right upper eyelid. On slit-lamp examination, moderate injection and temporal chemosis were noted in the right eye. There was a 4 x 4-mm area of infiltrate with an overlying serpentine epithelial defect measuring 4 mm vertically x 2 mm horizontally at the superior and temporal infiltrate border. Scattered endoplaque with five areas of dense radial keratoneuritis were also seen (See Figure 1). Examination of the left eye without staining showed multiple inactive scattered peripheral scars. Dilated funduscopic examination of both eyes was normal.
For Diagnosis & Discussion, click here.


