A 41-year-old Indian male presented with a four-month history of progressively blurry vision in both eyes. He initially noted decreased vision in his left eye at near and at distance, followed by similar changes in his right eye several weeks later. He also reported new floaters in both eyes. He denied associated headaches or eye pain, flashes of light, recent trauma or illness, and denied similar episodes in the past. He was first evaluated by an outside ophthalmologist, diagnosed
 |
Medical History
Past ocular history was notable for glaucoma diagnosed 10 years earlier and controlled with dorzolamide 2%/timolol 0.5% and brimonidine 0.15%. He had no significant past medical history, and the review of systems was unrevealing. He took no systemic medications and had no known drug allergies. His family history was noncontributory. He denied tobacco and alcohol use. He had emigrated from Chennai, India, four years prior to his presentation.
Examination
Ocular examination demonstrated a best-corrected visual acuity of 20/40 OD and 20/50 OS. On pupillary exam there was no relative afferent pupillary defect, but the right pupil was noted to be sluggishly reactive. Extraocular motility was full in both eyes and visual fields were full to confrontation in both. The intraocular pressure was 9 mmHg OD and 12 mmHg OS.
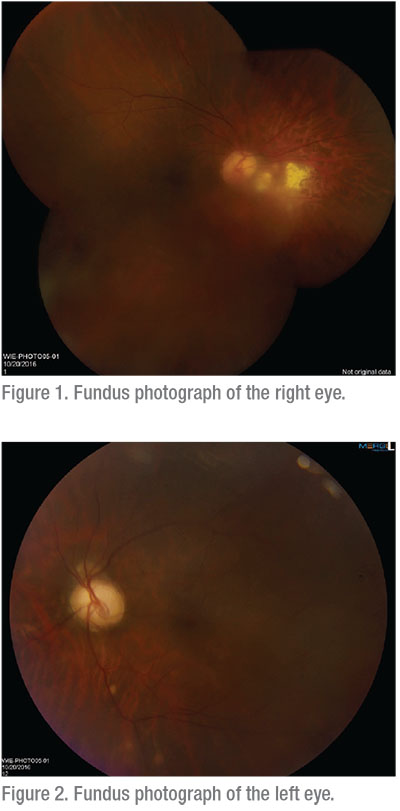
On anterior slit lamp examination there was 3+ cells in the anterior chamber OD and 2+ cells in the anterior chamber OS. There were no keratic precipitates or synechiae. Funduscopic exam of the right eye (See Figure 1) demonstrated 2 to 3+ vitreous cells with moderate vitreous debris. The optic nerve was pink and healthy, the vessels were normal caliber without vasculitis and there was no macular edema. There was chorioretinal scarring nasal to the disc from 2 to 4 o’clock, and scattered snowballs were seen in the periphery. Fundoscopic examination of the left eye (See Figure 2) revealed 1+ vitreous cells with moderate vitreous debris and scattered snowballs. The optic nerve and vessels appeared normal, but there was macular thickening without retinal hemorrhage.
Click here to view the Diagnosis & Discussion.


