“Throughout the whole course of medical history there have been difficult patients,” says John Pinto, president of J. Pinto & Associates Inc., a well-known ophthalmic practice management consulting firm. “Today, however, they’re more educated and much better-informed because of the Internet. Back in the 1970s, only one American out of 10 had a college degree. Now about one-third of all Americans are college-educated; and that, combined with having an encyclopedia in your pocket, means that if you are a difficult patient or someone who is going to dispute the doctor or ask a million follow-up questions, you are well-prepared to do so.
“The number of ‘difficult’ patients you have will depend on where and how you practice,” he continues. “Classically, if you have a LASIK practice, a plastics practice offering elective procedures or a practice located in urban centers, you’re going to have more patients who are better educated and more argumentative, bringing new facts to the table and having questions for you.”
Mr. Pinto points out that part of the reason for an increase in “difficult” patients is the changing nature of ophthalmology. “It’s certainly true that patients are asking more questions than they did before, but you also have to realize that ophthalmology has moved into more elective or quasi-elective spheres such as refractive surgery, advanced IOLs and even optical dispensing,” he says. “In these areas the patient knows whether his eyes seem right or not. He knows whether he can see better than he did before. This is not like general medicine or surgery where the treatment provided by the doctor might not be discernable by the patient as having fixed a problem. After many of today’s ophthalmological procedures, the patient can decide for himself whether the doctor fixed him or not.
|
“Of course, this applies to every service provider, whether you’re a waitress or chef or barber,” he notes. “But the potential difficulty of being in this position makes it important to be a witnessing presence, to stand apart from yourself and watch how you’re responding to those patients. If your response is a source of discomfort and loss of career satisfaction, then you owe it to yourself and your practice to do something to help you deal with these situations differently.”
Information From the Web
There’s no question that much of what makes difficult patients seem more difficult today is their unfettered access to the Internet. James J. Salz, MD, clinical professor of ophthalmology at the University of Southern California, Keck Medical School, and in private practice in West Los Angeles, notes that it’s not just young people who are using the Internet to research their condition. “Today our Medicare patients in their 70s and 80s have smartphones or iPads and use them to do Google searches,” he says. “So individuals who might have been intimidated by a desktop or laptop computer can get exactly the same information from a less-imposing device, which they might also be using to read a book.”
Obviously, the most common source of trouble is a patient coming in with incorrect information. Stephen Pascucci, MD, FACS, founder of Eye Consultants of Bonita Springs, in Florida, says this happens fairly often, and he believes the best way to deal with it is to be very confident, knowledgeable and well-informed about what you think is best. “For example, one new patient of mine was aware that she had astigmatism and came in believing she needed a toric lens,” he says. “She did need cataract surgery, but she didn’t have much astigmatism, and it was a type that might help her with reading after surgery. I showed her the topography and explained why her existing astigmatism wasn’t necessarily a bad thing and why I thought a toric lens wouldn’t work to her advantage. She understood there was a rationale for my disagreeing with her.”
He also notes that one of the best ways to manage patients coming in with incorrect information is to educate your staff so that patients’ questions can be answered and misconceptions corrected. “Your staff needs to feel very comfortable answering questions,” he says. “This enhances the patient experience and saves the doctor a lot of time, because most of the issues are sorted out before the doctor sees the patient. This also makes sense because in my experience patients are much more comfortable with the staff than with the doctor. They’re more apt to ask my staff their questions, and they seem to believe what my staff tells them, as if it’s gospel. In our practice that may be partly because we focus on letting the staff develop a relationship with each patient.”
Dr. Salz agrees that patients sometimes glean incorrect information from the Internet. “That’s OK,” he says. “If they’re misinformed it only takes a few minutes to straighten them out. A patient may come in very worried because he has a black spot in his field of vision. After surfing the Web he concluded that he has macular degeneration or a detached retina, when it’s really just a floater. Patients are often misinformed about cataracts too; they sometimes come in thinking they need surgery right away, when their vision is still quite good and they won’t need surgery for a while. I see this as a great opportunity for us to teach them and relieve their fear. So I’m in favor of patients searching for information on the Web.
“I’m sure it’s possible to get the wrong diagnosis or treatment ideas searching the Internet,” he adds, “but I haven’t had any patient come in having instituted some kind of treatment that was incorrect based on information they found on the Internet. In fact, they often find the right information. We have patients who have correctly diagnosed that they have a chalazion. They look it up, see what it is and find out that one of the best treatments is putting hot compresses on the eye. So they’re already doing the right thing when they see us.”
Vance Thompson, MD, assistant professor of ophthalmology at the University of South Dakota School of Medicine and founder of Vance Thompson Vision in Sioux Falls, S.D., believes that, in general, patients getting information from the Internet is a good thing. “The most common cause of a patient being unhappy is unrealistic expectations, and for that reason I don’t think it’s possible to have too much education,” he says. “Patients may come in asking about the negatives, but I don’t think anyone has ever asked me about something that didn’t actually happen at some point. So they’re reading about real concerns; they just have a hard time putting them into perspective, and as a result they may be much too worried about them. If we put those concerns in the proper context, and document the fact that they read about it and that we had a discussion about it, I think it helps our patient education—and also helps us medico-legally.”
Dr. Thompson acknowledges that some patients can’t be dissuaded from their fears. “If a patient reads frightening things on the Internet, those fears can win out, even if he meets with a balanced doctor who provides balanced information about his concerns,” he says. “But if a patient like that doesn’t proceed with the surgery, that’s probably for the best. In that situation the patient isn’t willing to believe the doctor, so that might be a patient you wouldn’t want to operate on in any case.
“The reality is, patients are getting information from the Internet, and we really don’t have a choice but to embrace it,” he concludes. “Are there sources of information that are too positive or negative? Sure. But it’s the same thing with word of mouth; a patient might run into an acquaintance or a doctor who is too positive or negative about a procedure and take the comments out of context. So being somewhat misinformed is not really a new phenomenon. It’s just that information in general is now much more accessible. In any case, it’s requiring us to embrace patient education at an even deeper level, and in general, I think that’s a good thing.”
Impatient Patients
One reflection of today’s “instant gratification” culture is patients being quicker to anger if they have to wait more than a few minutes to see the doctor. “That’s especially stressful for the staff,” notes Dr. Pascucci. “They get the brunt of patient complaints about this. It also drives the staff a little crazy that patients tend to be nicer when in the presence of the doctor. A few patients do argue with me, but many of them just go after the staff. They think the doctor is the one who has to take care of them, so they don’t want to make him or her upset.”
Dr. Pascucci says that when a patient does get upset because of an unusual delay, he and his staff go out of their way to apologize and try to neutralize any negativity. “Recently, a patient with a 2:00 p.m. appointment was told by the surgery center that the appointment was at 1:15, so she showed up early and had to wait a long time to see me,” he says. “The technician told me what had happened, so I walked in and apologized for the confusion. I was doing her second eye the following week, so I told her we’d make that appointment right now for whatever time she wanted, and I’d make sure she saw me at that time. That immediately neutralized her anger. The point is that you have to be prepared to deal with anger diplomatically and not just blow it off. Your patients want you to treat them like they matter.”
|

Dr. Thompson has invested a lot in that philosophy. “We built a brand new 34,000 sq. foot facility about 18 months ago,” he says. (See picture, facing page.) “I also had my CEO trained by Jim Gilmore, one of the authors of the book The Experience Economy. I want the patient experience to permeate every step of a patient’s journey through our practice.”
Simple Waiting Room Strategies
Of course, not every practice can go to such lengths to improve the patient experience. Mr. Pinto offers a number of simpler strategies for minimizing confrontations with difficult patients when waiting times get longer than usual. “The classic service-enhancement tools come to mind,” he says. “For example, manage patients’ expectations when they check in. Tell patients if you’re running behind—or that everything is on time, if that’s the case. The front desk person might say, ‘We normally like to get our patients in and out of here within an hour or less, but we’re running a little bit behind today, so your total time in the clinic is probably going to be more like an hour and 20 minutes. Is that going to work out OK for you?’ Saying this helps to minimize the number of disgruntled patients you have to deal with.
“Second, to the extent possible given the current economics of your practice, make the waiting period a pleasant experience for the patient,” he continues. “Set up your physical plant to be soothing and calming for your patients. Have an alcove here and there where patients can quietly read if they want to or watch TV if that’s their preference. (Admittedly, it will be easier for large practices to do this.) People want comfortable, diverse waiting areas that don’t force them to touch other patients and allow them a bit of respite. Pleasant lighting is very important. I’ve even worked with practices that have used aromatherapy experts to make sure that there’s a spa-like ambience. At the least, the front desk staff should keep the reception area clean and tidy.”
Mr. Pinto notes that it’s important to have refreshments available for patients in case you do run behind. “It doesn’t cost much at all to have small bottles of water in a glass-fronted refrigerator in the waiting room,” he says. “It doesn’t cost much to put out some granola bars in mid-morning when stomachs are starting to grumble. Just having a bowl of apples or a few snacks on a table with a coffee urn makes patients feel more at home, even if they don’t avail themselves of that courtesy. It’s a nice gesture. If you see a bunch of apples at the front desk of a hotel, they didn’t put them there to feed you. They put them there as a welcoming gesture, to give you a sense that they care about your well-being. Also, if a patient is waiting an unusually long time, a staff member should walk over and ask if the patient needs anything or would like a refreshment.”
Mr. Pinto points out that it’s important to know what patients will normally tolerate. “Many studies have shown, for example, that patients will usually be fairly patient until about 19 minutes of waiting time has passed. When 20 minutes hits, an alarm goes off in the typical patient’s mind, and they start to be unhappy. So it’s not a bad idea to make it your goal to manage the throughput of patients so you can keep the primary wait at or under 19 minutes. If you realize you can’t manage that, for whatever reason, be sure to let patients know as soon as they come in.
“Ultimately, you need to be aware of what the normal limits are for transit time and waiting time in your type of practice, and do everything possible to stay within those norms,” he adds. “That means making sure you’re not trying to jam too many patients through a fixed-capacity clinic. I see many practices where, in an effort to keep up economically, the doctors have taken a clinic/staff cohort and infrastructure that’s suitable for 50 patients a day and tried to jam 70 patients through every day. Obviously things will bog down if you do that, and it’s tougher on the staff, the doctor and the patients. So it’s important to be intentional about where you’re trying to go with a practice, and not create problems for yourself.”
Minimizing Misinformation
One of the best ways to avoid patient problems resulting from misinformation gleaned from the Web is to be proactive about reaching patients with accurate information. These strategies will help:
• Send preop materials designed to offset potential misinformation. “I try to create really good preop education materials,” says Dr. Thompson. “The current environment requires us to really bring our A game with what we produce so that it’s balanced and easy to read, well-organized and not overwhelming. That way patients get to hear our side of the story too.”
• Direct your patients to websites that will provide accurate information. Dr. Thompson points out that if patients are going to search the Web anyway, you can forestall a lot of trouble by pointing them in the right direction. “I always talk with my patients about good websites to visit,” he says. “I’m a big fan of allaboutvision.com and the Academy’s [American Academy of Ophthalmology’s] patient education website, geteyesmart.org.”
• Aim your social media exposure at all of your patients. “Even our senior patients are using social media these days,” notes Dr. Thompson. “We’re amazed how many seniors are doing email and social media and are on Facebook. Five years ago I don’t think that was true, but we’ve definitely seen a shift.”
• Make sure your practice’s website is information-rich. “This is not only a good way to offset less-accurate information found on the Web, it’s also an opportunity to convey your practice philosophy,” says Dr. Thompson. “That can do a lot to inspire patients to come to see you and stay with your practice.”
|

“It’s an amazing story, because the FDA studies that we did to get PRK and LASIK approved didn’t require demonstrating the level of postoperative vision the military wanted,” he says. “The military had to be convinced that if your eye had LASIK, it would perform in every way as well as a patient who was born with 20/20 vision. As I tell my patients, it’s one thing for you to see well enough to drive down the 405 freeway in L.A.; it’s another thing to see well enough to land a Navy jet on an aircraft carrier at night out in the ocean when the carrier is moving. That’s a whole different level of vision. Seeing this story on my website really helps when patients are a little apprehensive about LASIK. Once they see that it’s widely done for pilots in the Navy and Air Force and now approved by NASA for astronauts, they’re a lot less worried.”
• Let patients know that if they’re concerned about anything they find on the Internet, you’re available to talk. This will help prevent patients from simply sitting and fretting over negative information they encounter on the Web, notes Dr. Thompson.
• If patients haven’t seen the information you’d like them to see before they come in, be prepared to provide it while they’re waiting. “We have iPads in our waiting rooms,” says Dr. Thompson. “If a patient hasn’t seen our materials, we ask the patient to look at them while waiting. This can save a lot of time correcting misinformation and explaining options during the exam, and facilitates the conversation by getting them as close as possible to my level of knowledge so they can make a balanced decision.”
Get Your Staff Onboard
Once patients come into your practice, be prepared to deal with any disagreements or misunderstandings that may be waiting to arise.
• As much as possible, have the same staff member tend to the same patients. Dr. Pascucci says this helps create a bond between the patient and the practice. “If one of my techs has assisted Mr. Smith or Mrs. Jones in the past, we do our best to ensure that the same person works with him or her again,” he explains. “When a patient sees the same technician at every visit, she develops a relationship and a level of trust. I recently gained a new patient because the practice she previously went to got bigger and bigger, and not only did she see the doctor for shorter and shorter periods of time, she also said she never encountered the same staff member twice; at every visit she was greeted by a new person. She came to feel that she didn’t know anyone there, so she decided to find a smaller, more personal practice. A friend recommended our practice for that very reason.”
• Make sure all your technicians can answer a wide array of patient questions—and make sure their answers will match yours. “Their answers should be scripted,” notes Mr. Pinto. “That way, the answers they give to patient questions are always the same answers the patient would receive from the provider.”
Dr. Pascucci agrees, noting that it’s important for staff members to get their question-answering information from the doctor rather than from a consultant or by attending meetings. “If you take your staff with you to meetings and let them listen, they’ll be picking up someone else’s viewpoint and prejudices,” he notes. “For example, they may end up favoring or disliking a specific lens or treatment approach. It’s more useful to encourage them to listen to what you say to your patients. If there isn’t enough time for your techs to be in the exam room observing and listening, this should be dealt with after the patient leaves. In our practice the staff is encouraged to ask what I recommended and why. Over time they become quite knowledgeable, and their knowledge is consistent with mine. That means that regardless of which staff member a patient asks about something, the answer will be the same.”
• Consider hiring a lay educator. “If your practice draws in many patients who are better educated and/or more argumentative, one solution is to allow more time to manage such patients. However, that’s tough in the current economic climate,” notes Mr. Pinto. “An alternative is to have a high-functioning lay educator in the practice who can step in when patients are taking up a lot of time. You can personally answer the first couple of questions, and then turn the patient over to your educator for questions #3 through #45. It’s not uncommon for practices with a large surgical volume to have a surgical counselor serving as a patient educator.
“You have to arrange to deal with whatever kind of patient population you have,” he adds. “To use a metaphor, if you practice where the snow falls, you’d better have a snow shovel. If you practice where the patients are really smart and well-educated, or disputatious—parts of New York come to mind—then you’re going to have to be prepared to answer questions personally or through a proxy.”
• Learn from your experience in other settings. Because a pleasant experience in the waiting room helps to diffuse anger, it pays to be open to new ideas about how to accomplish that. “When you go to the gym, the spa, the car dealership or the retail store, notice what they do to make you comfortable,” suggests Mr. Pinto. “You’ll come away with ideas for what you can add to your own clinic to make it a more pleasant experience for the patient, and ultimately make the patients more pleasant to be with when they’re in the exam room.”
Dr. Thompson agrees. “About 10 years ago we assembled 10 physicians from different practices under the direction of Jim Gilmore and Shareef Mahdavi, and began meeting periodically in different cities like Chicago, Cleveland and Washington, D.C.,” he says. “We spent time going into places that create a great customer experience, like the American Girl Doll store in Chicago. Then we’d go back to our meeting room and discuss what we’d learned and how it could be applied in our practices. We did this for two years, and we learned a lot about creating a great patient experience.”
Managing Confrontations
Despite your best efforts, some patients in some circumstances will end up in conflict with you or your staff. These strategies will help keep things under control:
• Have a practiced way for everyone on staff to respond to an upset patient. Mr. Pinto notes that doing a good job of managing difficult patients doesn’t just make work a lot more pleasant—it also prevents lawsuits. “As they say in malpractice insurance circles, patients don’t sue because of bad outcomes, they sue because of bad relationships,” he says. “Your practice should have a plan for how to respond when a patient is unhappy with a result. That way a bad mood or high stress level on the part of you or your staff won’t lead to a negative encounter.”
Should the staff receive special training in managing difficult patients? “I prefer not to delegate this sort of thing,” says Dr. Pascucci. “The staff will be given the psychologist’s viewpoint on everything, which may or may not agree with my viewpoint. So I choose to teach my staff how I would like them to behave when faced with a difficult patient. I got a lot of my ideas about how to manage this from reading a book about how the Ritz Carlton hotel trains its staff: The New Gold Standard by Joseph Michelli. In fact, one of our receptionists used to be the front desk manager of a nice hotel here in Naples, Florida. She treats our patients the same way she treated the hotel patrons. She says: ‘It will be my pleasure. Absolutely. No problem.’ Now, the rest of the staff has started talking the same way. They don’t want to seem less polite than her.”
• Remember that your staff will take their cue from you. Dr. Pascucci points out that the doctor’s example makes a big difference in how staff behave. “In general, the older staff members are better at managing upset patients than younger staff members, who tend to get frustrated,” he says. “But I believe that overall, the staff members take their cues from the doctor. If the doctor displays some degree of patience and manners and understanding, the staff will follow suit.”
• When you disagree with a patient, make sure to explain your reasons. “If you agree with the patient’s preconceived notion, tell him so; if you disagree, give him a reason,” says Dr. Pascucci. “Patients need to perceive your thought processes as being well-thought-out, logical and based on experience.”
• Break up a challenge by conceding the possibility that the patient may be right. “Whether you’re a provider or a staff member, when a patient has asked his fourth question or is trying to argue medical wisdom, the universal solvent is to politely say, ‘You know, you might be right.” That quiets him down and allows him to listen to whatever you say next, which might be: ‘However, the evidence in our practice experience has been that X is actually the case.’ Or: ‘However, things have worked out very well for the past 1,000 patients we’ve provided this procedure to.’ That will allow you to foreshorten the discussion.”
• If you often have a problem dealing with patients, have a staff member serve as a go-between. “If you’re the kind of doctor who is a great surgical technician but not so great with personal relationships, try to interpose a lay staff member between you and the patient—someone who can soften your touch,” says Mr. Pinto. “I have plenty of surgeon clients who really don’t like patients all that much. They adore surgery, they love medicine, they love solving patient problems, but they don’t like dealing with the human being behind that pair of eyes. So, they have staff members act as a lubricant between the patient and the cranky doctor.”
• Consider making yourself available via email. “I give every patient my personal email address, so if they have any questions preop or postop they can email me,” says Dr. Thompson. “All of my exam rooms have a stack of my business cards. It’s amazing how many of my senior patients email me. At the same time, abuse of this has been almost nonexistent.”
• If you need counseling assistance, get it. “The doctors who tend to get the most exasperated by difficult patients are those who are very insecure,” notes Mr. Pinto. “A self-assured, confident doctor is never defensive when a patient second-guesses his judgment or says ‘What about this medication or this treatment?’ It’s the doctors who are less secure professionally and thus more defensive who can spiral up into a tangle with these so-called difficult patients.
“If you bristle when a high-school-educated patient says, ‘Gosh doctor, I’m not seeing as well out of that eye you operated on as I thought I would,’ you probably would benefit from counseling,” he continues. “Some doctors become defensive easily, whether it’s when their 9-year-old daughter argues with them, or a shopkeeper asks about their motives or a patient or staff member asks a question that appears to defy their authority. If you feel a little tense when someone does that to you, that reflects a sense of insecurity. It’s very reasonable to ask yourself why that’s the case. If this is a frequent experience, it’s likely that you have an issue, not your patients.
 |
Making the Best of It
For a doctor in the 21st century, there’s no escaping the occasional encounter with a difficult patient—and the likelihood of that encounter does seem to have increased with the explosion of information access and increased expectations of instant gratification that have come with it.
“It’s a great frustration that in these days of tapering fees, rising costs and falling profits, we simultaneously have to up our game and provide better objective outcomes, as well as create better subjective impressions for our patients,” says Mr. Pinto. “But that’s the name of the game. And it’s not just happening in ophthalmology; it’s happening at every level. People have much higher standards today for restaurants and haircuts and hotel rooms. They have more options to choose from than every before. So we have to up our game accordingly.”
“This is a tough job,” adds Dr. Pascucci. “Many doctors who have been doing this for a long time are burnt out. But having an effective strategy for managing difficult patients can do a lot to lower the stress and make the work more palatable.” REVIEW
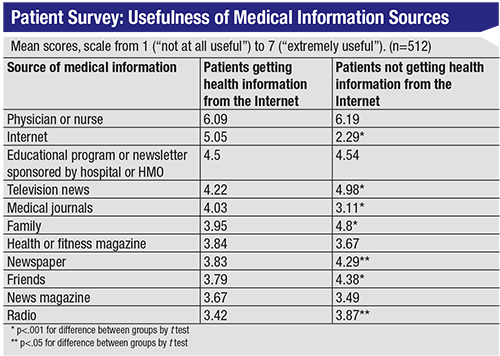
1. Diaz JA, Griffith RA, et al. Patients’ use of the Internet for medical information. J Gen Intern Med 2002;17:3:180-5.






