With that in mind, three clinicians who have done extensive research in this area share their experience and latest thinking on angle closure: how it happens; why it happens; and what clinicians can do to manage it to—hopefully—prevent vision loss.
A Major Health Issue
“Glaucoma is the second leading cause of blindness globally, and angle closure accounts for close to half of the blindness caused by the disease,” notes David S. Friedman, MD, MPH, director of the Dana Center for Preventive Ophthalmology, and the Alfred Sommer Professor of Ophthalmology at the Wilmer Eye Institute of Johns Hopkins University School of Medicine. “It’s less common than open-angle glaucoma, but a large number of population-based studies have shown that people who have angle-closure glaucoma typically have more severe damage than people who have open-angle glaucoma.
“Angle-closure glaucoma develops because the anterior part of the eye is crowded,” he continues. “That is reflected in many different measurements that we do. Also, the length from the front to the back of the eye in these patients, on average, is a little bit shorter. However, that doesn’t mean that a short eye will necessarily develop angle closure, or that people with longer-than-average eyes are immune to it. It’s really the way the anterior segment structures are positioned that causes the disease.”
Dr. Friedman notes that there’s a misunderstanding that in China narrow angle glaucoma is more common than open-angle glaucoma. “That’s not the case,” he says. “Angle-closure glaucoma is still less common. It’s just that angle closure is much more common than it is here. People used to say it was 10 times more common among the Chinese, which is also not true; it’s probably two or three times more common. In any case, because the population at risk is so large and aging, there’s a big public health issue developing.”
Categories of Closure
“Like open-angle glaucoma, angle-closure glaucoma comes in many forms,” notes Jeffrey M. Liebmann, MD, clinical professor of ophthalmology at New York University School of Medicine, adjunct professor of clinical ophthalmology at New York Medical College and director of glaucoma services at Manhattan Eye, Ear, and Throat Hospital and New York University Medical Center. “It’s not just one disorder—a series of different conditions can lead to anatomically narrow angles, angle closure and acute angle-closure attacks. Given that fact, the most important thing doctors can do is develop a systematic approach to the angle-closure glaucomas, just as they would for primary open-angle glaucoma, to try to determine the cause of the angle closure. Once you know the cause, you can direct the treatment to that cause.”
|
“Another widely used term I think we should avoid is ‘occludable angle,’ referring to an eye we think might occlude,” he continues. “In reality, we have very little understanding of who occludes and who will have an acute attack. I think using accurate names to describe what we see is important because when we give something a name, we often then feel compelled to act on it. If it sounds like it might kill you, you’ll probably feel that you need to do something, when in fact it would make more sense to say, ‘I don’t really know what’s going on, so let’s keep an eye on it.’ ”
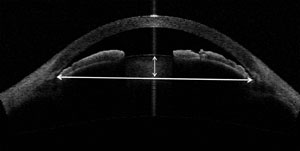
In terms of anatomy, Dr. Friedman says a few factors seem to be key. “Some individuals have their lens very anterior to the scleral spur, pushing into the anterior segment,” he says. “We can measure that by marking the scleral spur and then seeing how much farther forward the lens is, which we call lens vault. A greater-than-average lens vault can be the dominant factor in closing the angle.” (See example, above.)
Dr. Friedman says he now prefers to divide angle closure patients into four major categories. “The largest category is people who are anatomically narrow—they look closed, but if you press on the eye with gonioscopy you can open the angle,” he explains. “There’s no scarring and the pressure’s normal. These eyes raise our suspicions, but there’s no apparent crisis. The second category is a group that has similarly narrow angles but also has synechiae in the angle and/or high pressures. (See example, p. 26.) We consider these individuals more worrisome, as they have the appearance of early disease development, although we don’t have a lot of natural history data on this group. The third category is those who clearly have glaucoma and closed angles. Finally, there’s a fourth group; those who present with an acute symptomatic attack of angle closure and high eye pressure. This is the simple new approach to categorizing these patients that we’ve been using.”
Causal Factors
In the majority of cases, angle closure in these patients is attributed to pupillary block and addressed by laser iridotomy, which reopens the angle. However, Dr. Liebmann notes that a number of other causes can underlie angle closure.
“In patients with plateau iris, the ciliary body configuration is abnormal,” he says. “The abnormally positioned ciliary body physically holds the peripheral iris to the trabecular meshwork. When laser iridotomy is performed in plateau iris, the angle usually opens only a very small amount and there is persistent appositional closure of the iris to the meshwork. This can be seen during indentation gonioscopy. If the iris is still touching the trabecular meshwork, you should then determine whether or not the patient requires further intervention such as a peripheral iridoplasty.
Fortunately, relatively few patients will require that.”
Dr. Friedman has mixed feelings about categorizing a patient as having plateau iris. “I look at angle-closure mechanisms as being multifactorial,” he says. “The iris might be thick or have an anterior insertion; the ciliary body could pushing the iris upwards. A number of factors probably play a role in angle closure, so labeling one case as plateau iris and another not seems like a little bit of an artificial construct. I think a mix of components is likely to be responsible.
|

“When we looked at clinic patients with angle closure to identify plateau iris using ultrasound biomicroscopy, very few people had plateau iris in all four quadrants,” he continues. “Most of them only had it in one or two quadrants. Furthermore, a lot of people who had plateau iris before iridotomy didn’t have it after, and a lot of people who didn’t have plateau iris before iridotomy did have it after. I think there are various mechanisms at play, so you can’t dismiss pupillary block as being a component even when you think it’s a case of plateau iris. That’s why I still emphasize doing an iridotomy in angle closure, as a necessary part of the treatment, regardless of the appearance of plateau iris.”
Dr. Liebmann notes that causes of angle closure may also lie farther back in the eye. “Disorders of the lens can cause angle closure, including enlargement of the lens as the cataract process advances,” he says. “In this case, the physical size of the lens is pushing the iris into the trabecular meshwork. Closure could also happen if the lens is subluxed or loose. The most common cause of zonular laxity is exfoliation syndrome; while exfoliation is a common cause of open-angle glaucoma, 10 percent of all patients who have exfoliation syndrome will have an angle-closure glaucoma component.
“Causes can also lie in the posterior segment,” he continues. “You can have angle closure related to disorders of the vitreous and the retina, and patients can develop angle closure after scleral buckling surgery. Still another angle closure currently of interest to doctors is malignant glaucoma. This form of angle closure, most often occurring after intraocular surgery, is characterized by flattening of the anterior chamber and high intraocular pressure; it’s relieved by rupturing the anterior hyaloid face using the YAG laser or vitrectomy. The pathogenesis of this disorder is an area of intense discussion among glaucomatologists. Finally, there are other more unusual potential causes of angle closure, such as ciliary cysts, but these are relatively uncommon.”
Diagnosis: Gonioscopy
In terms of clinical diagnosis, the three approaches most commonly used to examine the angle are gonioscopy, ultrasound biomicroscopy and optical coherence tomography. “I do both gonioscopy and OCT, but the reference standard is gonioscopy,” says Shan C. Lin, MD, professor of clinical ophthalmology and co-director of glaucoma at the University of California San Francisco. “Unfortunately, gonioscopy is currently not done at least half the time in patients who have glaucoma or glaucoma suspicion, and those are the ones who really need gonioscopy. Arguably, everybody deserves at least one gonioscopic exam in order to really determine what’s going on with the angle.
“As to whether a patient needs treatment,” he adds, “in the United States the criterion is that if you can’t see the posterior trabecular meshwork for 180 degrees or more, that’s considered to be an occludable angle and the patient should receive prophylactic laser.”
Dr. Friedman notes that one reason identifying angle closure is still a challenge is that gonioscopy is subjective. “It’s also uncomfortable for patients, and doctors frequently don’t perform it,” he points out. “We’ve looked at charts across the United States from health-care plans, and the charts of at least half of the people diagnosed with glaucoma contained no evidence that the patient had undergone gonioscopy. But doctors can’t really know that they’re dealing with open-angle glaucoma unless they look at the angle to see whether it’s open.”
“Gonioscopy is the single most important thing the ophthalmologist can do to detect angle closure,” agrees Dr. Liebmann. “It allows us to determine whether the angle is just narrow, or whether there is actual apposition of the iris to the trabecular meshwork. We recommend that every patient—at least the first time he’s examined by an ophthalmologist—have gonioscopy. Indentation gonioscopy does not require any coupling gels and it only takes a very short time to perform.
“One of the key things about gonioscopy is to perform it in relatively dark conditions,” he adds. “If a bright slit beam is directed through the pupil, the pupil constricts and the angle opens. Gonioscopy should be performed with the room lights out, using a small beam of light directed through the gonioprism mirror to look at the angle. Care needs to be taken to avoid shining it through the pupil. As the pupil dilates with darkening room conditions there’s a better chance of making a diagnosis of angle closure if it is present.”
Diagnosis: Imaging the Angle
“In recent years we’ve done a lot of research on the mechanisms of angle closure because there are a number of excellent imaging technologies now available that have allowed us to see much more of what’s going on,” notes Dr. Friedman. “The first technology that helped in this regard was ultrasound biomicroscopy, which appeared 20 or 25 years ago. That allowed one quadrant of the filtering part of the eye to be seen in tremendous detail, giving us a lot more insight into the angle-closure mechanism. More recently we’ve had the anterior segment OCT devices, which allow us to see the entire anterior segment from side to side in slices. That provides a lot of information about the relationship of various structures to each other. Even more recently, the development of three-dimensional imaging has allowed us to see the whole anterior segment as a unit. All of this is allowing us to learn much more about the mechanisms and causes of this condition.”
Dr. Friedman observes that one of the benefits of imaging technology is that it can often simplify complicated information through algorithmic analyses. “For example,” he says, “we have a manuscript in submission describing software that can take a single slice of an anterior segment OCT and say with 95-percent accuracy whether if you do gonioscopy you’ll find the angle to be open or closed. That’s with minimal physician input. The only thing you need to do to make the algorithm work is identify the scleral spur in the angle images. Of course, that identification can be an issue with some technologies—you can’t always identify the scleral spur in an image. But tests of this algorithm done in two populations found that it was very accurate. We hope that at some point this will lead to a Star Trek-style device that you can simply place over the eye; it will tell you whether the angle is open or closed. I think that’s where we’re headed.”
Despite his optimism, Dr. Friedman notes that use of imaging technology currently has limitations. “Is there information in these scans? Certainly,” he says. “Do we have enough data on which to base clinical recommendations from various tests like these? I don’t think so, although we’re working in that direction. Just because you have the technology, it doesn’t necessarily mean that you’re going to do better applying it in the clinic.”
Dr. Lin notes that OCT technology provides a more objective evaluation of the angle. “In a way, it’s a verification of my gonioscopy,” he says. “I’d say that most doctors don’t use it for assessing the angle, probably because the stand-alone device that’s specific for that purpose—the Visante OCT from Zeiss—is quite expensive. But in recent years several manufacturers have incorporated anterior segment imaging into their standard Fourier domain OCTs, which should make this more accessible to clinicians.
|

Dr. Lin notes that one of the most useful pieces of information obtainable with OCT is lens vault. “This is the factor that seems to be mathematically most correlated with angle closure,” he says. “A group in Singapore looked at all the factors associated with angle width in their population. They found that, statistically, lens vault was the most closely correlated, even taking into consideration other factors such as iris thickness and area and anterior chamber width.1 Of course, you may be able to tell that lens vault is significant just by looking at the patient or by doing gonioscopy, but AS-OCT allows you to quantify that.
“Despite the advantages of OCT, many doctors still see gonioscopy as the gold standard,” he adds. “You could argue that it has some advantages beyond the cost issue, some of which are related to the disadvantages. For example, when doing gonioscopy you can end up pushing on the eye and altering the anatomy. But that can also be used as an advantage, to see whether the eye has peripheral anterior synechiae, for example. Being able to do that can lead to a different classification of the patient and different management.”
A Question of Intervention
“For most patients with angle closure, it’s a slow disease process,” says Dr. Liebmann. “At first the iris intermittently touches the trabecular meshwork; then you see more chronic apposition, pigment deposition on the trabecular meshwork and synechiae formation. Only then does the pressure start to rise. As far as an acute attack, there’s no way of determining who’s going to have one or when it will occur.
“Once the pressure rises in angle closure, the cat’s out of the bag and the meshwork has been significantly damaged,” he notes. “The pressure usually rises slowly over time in most patients who go on to develop chronic angle-closure glaucoma, but in some patients it fluctuates with the position of the iris. Widely fluctuating IOP in a patient previously thought to have open-angle glaucoma could be indicative of an angle-closure process.
“For me, the time to intervene is when the iris is touching the trabecular meshwork,” he continues. “Once angle closure is identified we recommend laser iridotomy to relieve the pupillary block component of the disease process for all those patients, regardless of whether they have a secondary cause of angle closure. On the other hand, we don’t usually intervene when the angle is narrow but open. In rare cases there are patients in whom we don’t see apposition, but the angle is slit-like and other conditions are present that might require frequent dilation (e.g., diabetes or macular degeneration); laser iridotomy might be indicated in selected cases.”
Dr. Friedman is a lead investigator on a trial taking place in China to determine whether or not iridotomy is beneficial for people who are anatomically narrow but have no scarring and have normal pressures. “We’ve randomized treatment to one eye, leaving the other eye untreated in more than 900 people who look suspicious,” he explains. “There’s another similar project in Singapore that I’m co-investigator on; that one involves a smaller number of subjects, but has been going on a little longer. The findings produced by these studies will be very important for public health purposes. The question we hope to answer is: Should we be doing an iridotomy—something potentially harmful—in all of these people, when nearly 20 percent of all people over the age of 50 in China have this finding? That’s an enormous number of people.”
|

The Cataract Surgery Option
“After you do an iridotomy, about 30 percent of eyes still have narrow or closed angles,” says Dr. Lin. “The primary reason, in several studies, has been plateau iris; this acts as a secondary mechanism keeping the angle narrow or closed. On the other hand, recent studies have shown that even in people with plateau iris, everybody opened up after cataract surgery.2,3 Therefore you’d surmise that cataract surgery would improve eye pressure and help prevent angle-closure glaucoma in these patients.
“Whether to do cataract surgery as the primary surgery for people who have primary angle-closure glaucoma is a hot-button issue,” he notes. “A few years ago we published a paper in which we looked at non-glaucomatous patients who had cataract surgery.4 We found that the amount the angle opened up correlated proportionally to the amount that the eye pressure went down. That suggests that the main mechanism by which cataract surgery lowers eye pressure is allowing the angle to open up, which makes sense.
“In fact, we recently submitted a paper on a case series of clear lens extractions for angle-closure glaucoma,” he continues. “We had five angle-closure cases at our county hospital where the pressures were high and the patients were on maximum medications; if left untreated they would almost certainly have needed glaucoma surgery. A trabeculectomy would have carried a high risk of complications, so we decided to proceed with clear lens extraction. Four of the five cases improved; one remained unchanged. That would seem to suggest that this is a reasonable alternative for treating angle-closure glaucoma, especially in comparison to a significant glaucoma surgery that has a high chance of failure.”
“There’s good evidence that removing the lens causes the intraocular pressure to drop in some people with angle closure,” notes Dr. Friedman. “It may be that the people that have lens vault as a dominant factor are the ones who need cataract surgery to help get the pressure down. Those who have cataract surgery and don’t have much eye pressure lowering may have other angle-closure mechanisms having more to do with the location of the ciliary body or the configuration of the iris.”
Dr. Friedman feels there may be a bit of excessive optimism about using cataract surgery to treat angle-closure glaucoma. “The lens is clearly a very important part of angle closure, and if you remove the lens, you eliminate angle closure,” he says. “However, that’s not the same as curing the glaucoma.
“In individuals who have had chronic angle closure longer-term, taking out the lens doesn’t always lower the pressure that much,” he continues. “It does seem to work if you start with a higher pressure, or if you’ve had an acute attack recently, in which case it’s definitely indicated and is beneficial. But the trials that have looked at more chronic forms of glaucoma find that just removing the lens provides only some benefit; it’s not the be-all and end-all at this point. I think there may still be room for additional therapies at the time of cataract surgery, especially as we get better at some of the newer outflow procedures.”
Dr. Friedman notes that there’s also the issue of risk. “Cataract surgery is effective and generally safe, but it’s not perfect,” he points out. “A small number of people get endophthalmitis and lose vision, and 1 or 2 percent have significant negative outcomes like macular edema or retinal detachment after cataract surgery. So if you’re considering applying this very widely and very early, you need to be a little cautious. In fact, there’s a very large clinical trial called the EAGLE trial being done, centered in Aberdeen, Scotland. They’re taking out clear lenses in people around the world who don’t have much cataract, to see whether that’s an effective way to treat angle-closure glaucoma.”
New Thoughts on Causes
In recent years, several new observations have been made regarding angle closure that may eventually help explain why some patients have the problem and others don’t. For example, work done by Harry Quigley, MD, and colleagues, including Dr. Friedman, has shown that the iris is a sponge, rapidly losing half its volume during dilation, thus avoiding “bunching up” and closing the angle. Eyes with angle closure, however, lose less volume when dilating than eyes without angle closure.5,6
“I definitely think that there are dynamic factors that play a role in who does and doesn’t have angle-closure problems,” says Dr. Friedman. “Some of my earliest research showed differences in the pupil’s response to light and dark. For example, in eyes with closed angles the pupils open less in response to lower light or pilocarpine. So there’s something about the physiology of the structure in the front of the eye in these individuals that alters that responsiveness.
“There’s no question that the iris has to lose some fluid when it jams itself into the angle during dilation,” he continues. “One of the hypotheses about this is that the iris in narrow-angle patients may have a different conduction of fluid in and out, and there’s some very good research showing that this is the case. So I think the sponge theory is legitimate, although we need a little more basic data to show exactly how that works.
“Unfortunately, for now, the static aspects of angle closure are easier to quickly capture, analyze and think about,” he adds. “And even if the iris behavior does differ in these patients, it’s not clear whether knowing that will help us manage the disease.”
Another avenue of exploration is centering around the discovery that choroidal expansion might be a factor in angle closure; choroidal effusion, measured by UBM, was found in 58 percent of eyes that underwent an acute angle-closure attack; 23 percent of fellow eyes; 20 percent of eyes with primary angle closure but no acute attack; and 1 percent of eyes with open-angle glaucoma.7
“It’s an interesting idea and it makes a lot of sense that it could be part of the causal mechanism,” says Dr. Friedman. “Harry Quigley has done a body of research that supports this, and given that imaging the choroid is not easy, the fact that he was able to show differences means that they’re likely to be real. The challenge will be figuring out how to use that information clinically.”
“I think these ideas that are sort of outside the box are great,” says Dr. Lin. “They could very well be correct. However, it’s too early for this to be of much use in the clinic. To measure these things will require advanced technology, and even if we measure the iris or choroid, how will it help us directly diagnose angle-closure glaucoma? We’ll still need to do gonioscopy and look at the angle. I suspect it will end up being like corneal thickness. Corneal thickness doesn’t tell you if a patient has glaucoma, but if a patient does have a thin cornea, your ears perk up a little bit and you look a little more carefully.”
Angle Closure in the Clinic
Based on their experience, Drs. Friedman, Liebmann and Lin offer these suggestions:
• Always consider the possibility of angle closure. “I think there’s a lot more angle closure in our clinics than people realize,” says Dr. Friedman. “So the first step is to always look for it as a possibility. If the patient flow in your clinic doesn’t permit everybody to be gonioscoped, look at the limbal anterior chamber depth, because that’s a very easy way to tell that an angle is likely to be narrow. If you look at the limbus and the iris is very close to or touching the cornea, you know there’s not a lot of angle opening. At a minimum, everybody should be doing that.”
|
• Be aware of demographic and biometric risk factors. “For example, angle closure is more common in smaller eyes,” says Dr. Liebmann. “Patients with hyperopia are at greater risk—and the greater the hyperopia, the greater the risk. Some ethnic groups are at greater risk, including people of Chinese ancestry and people of African descent.”
• Learn to be facile with the gonioprism. “Once you do that, you can perform gonioscopy in 15 seconds,” notes Dr. Liebmann. “It’s not a difficult thing to do.”
• Don’t just do an iridotomy and assume all is well. “In the majority of cases, the first line of treatment is to do a peripheral iridotomy, but it’s crucial to reassess these patients afterwards and see whether the angle is improved,” Dr. Lin points out. “If it isn’t, you have to think about what else you might do, and follow them closely. It’s true that many of these patients get relief after having a patent iridotomy, but almost 30 percent of them are still narrow afterwards. That’s almost a third who need to be reassessed.”
• If the patient has had an acute attack, perform cataract surgery. “The vast majority of patients who have had an acute attack of angle closure will benefit from cataract surgery,” notes Dr. Friedman. “It’s probably a good idea to do this about a month after the attack. It will decrease the likelihood that the patient will go on to develop high eye pressures and glaucoma.”
• Avoid trabeculectomy in these patients. “Trabeculectomy is fairly risky in angle-closure patients,” says Dr. Friedman. “If you don’t need to achieve too low a pressure, taking out the lens is a reasonable first option for many patients.”
Keeping It Simple
“Although some of the research is complex and there’s a lot we don’t yet understand, I like to keep it simple when I’m practicing,” says Dr.
Liebmann. “Keeping it simple means identifying that the angle is closed and then identifying the cause of the block.
“First, I determine whether the iris is touching the trabecular meshwork,” he continues. “Second, I determine the level of the block. Most often it’s pupillary block, so I perform laser iridotomy. Once you’ve done that, you’ve taken care of the vast majority of the cases; a patient only becomes challenging and complex when the angle remains closed. For the most part, you don’t have to get into the other mechanisms—the plateau iris, the posterior segment ones.
“In most cases, once you’ve performed laser iridotomy, management is similar to open-angle glaucoma,” he adds. “If the angle fails to open after iridotomy, other causes should be sought.” REVIEW
Drs. Friedman and Lin have received non-financial research support from Zeiss via the loan of equipment, but have no financial connection to the company. Dr. Liebmann has no financial interest in any of the technologies discussed.
1. Foo LL, Nongpiur ME, Allen JC, Perera SA, Friedman DS, He M, Cheng CY, Wong TY, Aung T. Determinants of angle width in Chinese Singaporeans. Ophthalmology 2012;119:2:278-82.
2. Nonaka A, Kondo T, Kikuchi M, Yamashiro K, Fujihara M, Iwawaki T, Yamamoto K, Kurimoto Y. Cataract surgery for residual angle closure after peripheral laser iridotomy. Ophthalmology 2005;112:6:974-9.
3. Nonaka A, Kondo T, Kikuchi M, Yamashiro K, Fujihara M, Iwawaki T, Yamamoto K, Kurimoto Y. Angle widening and alteration of ciliary process configuration after cataract surgery for primary angle closure. Ophthalmology 2006;113:3:437-41.
4. Huang G, Gonzalez E, Peng PH, Lee R, Leeungurasatien T, He M, Porco T, Lin SC. Anterior chamber depth, iridocorneal angle width, and intraocular pressure changes after phacoemulsification: narrow vs open iridocorneal angles. Arch Ophthalmol 2011;129:10:1283-90.
5. Quigley HA, Silver DM, Friedman DS, He M, Plyler RJ, Eberhart CG, Jampel HD, Ramulu P. Iris cross-sectional area decreases with pupil dilation and its dynamic behavior is a risk factor in angle closure. J Glaucoma. 2009;18:3:173-9.
6. Aptel F, Denis P. Optical coherence tomography quantitative analysis of iris volume changes after pharmacologic mydriasis. Ophthalmology. 2010;117:1:3-10.
7. Sakai H, Morine-Shinjyo S, Shinzato M, Nakamura Y, Sakai M, Sawaguchi S. Uveal effusion in primary angle-closure glaucoma. Ophthalmology 2005;112:3:413-9.