A 4-year-old Caucasian male with a history of intermittent exotropia, anisometropia and amblyopia of the right eye was referred to the Ocular Oncology service for evaluation of a pigmented iris lesion of the right eye. The lesion was first noted at 11 weeks of age by the child’s pediatric ophthalmologist and was thought to represent a benign nevus. The lesion was photographed and no growth was observed.
Despite patching of the left eye four hours daily since 6 months of age and full correction of refractive error, the amblyopia of the right eye failed to improve. This was presumed to be due to noncompliance with patching. Intermittent exotropia became more constant and at 3 years of age a 30-prism diopter exotropia was corrected with a 9.5-mm recession of the right medial rectus muscle. Following strabismus surgery, the patient was referred to Ocular Oncology by his strabismologist for evaluation of the pigmented iris lesion.
Medical History
The patient was born full-term via cesarean section following an uncomplicated pregnancy. He had a history of gross motor apraxia for which he underwent physical therapy, as well as a mild speech impediment for which he received speech therapy. He was otherwise in good health, with no history of major illnesses. He took no medications and had no known drug allergies. Family history was significant for a multiple relatives with various cancers including ovarian cancer, prostate cancer, thyroid cancer and malignant melanoma of the skin.
Examination
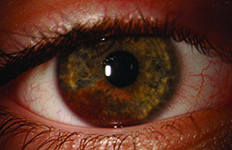
Ocular examination demonstrated a best corrected visual acuity of 20/400 OD and 20/20 OS. Pupils were equal, round and reactive to light with no relative afferent pupillary defect. Finger tensions were normal in both eyes. External examination was normal with no abnormalities of the skin or periorbital adnexa (See Figure 1). Slit-lamp examination revealed an ill-defined, darkly pigmented, vascular iris lesion extending from the pupillary margin to the angle and involving the 5 o’clock to 8 o’clock inferior region without associated feeder vessels (See Figure 2). Anterior segment examination was otherwise normal. Dilated fundus examination was performed in the clinic; however, due to poor cooperation, only limited views of the fundus were obtained.
|

Please click this link for diagnosis, workup, treatment and discussion.


