The Wills Eye Hospital Neuro-ophthalmology service was consulted to evaluate a 55-year-old male inpatient with the complaint of new-onset “crossed eyes.” The patient was driving his car in a convenience store parking lot and crashed his vehicle into a parked car at a speed of less than 5 mph. When police arrived at the scene, they noted the man to be confused as well as unsteady on his feet, and he was transported to a local hospital. The patient’s relatives were called to the hospital and noted his new-onset “crossed eyes.”
|
Medical History
Past medical history was significant for alcohol abuse and subdural hematoma requiring craniotomy after a fall four months earlier. The patient took no chronic medications. Family history was unremarkable.
Examination
The patient was afebrile with normal vital signs. He was disheveled in appearance, in no acute distress, but alert and oriented to self only. Uncorrected visual acuity was 20/50 in both eyes with near card; no afferent pupillary defect was detected, and color plates were full.
The patient demonstrated 15 prism diopters of esotropia in primary gaze at distance. Ductions in the right eye were full other than 70 percent abduction and 90 percent adduction. Ductions in the left eye were full other than 70 percent abduction and 90 percent adduction. Horizontal jerk nystagmus in left and right gaze and upbeating, torsional nystagmus in upgaze were noted in both eyes.
Anterior segment examination was only notable for 2+ nuclear sclerosis. Dilated fundus exam was within normal limits with no optic disc edema.
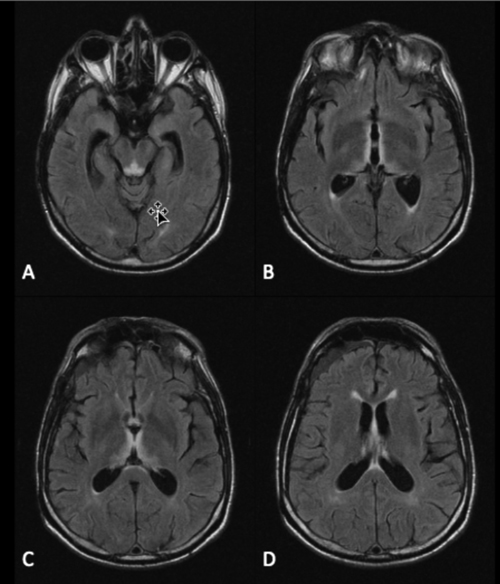
An urgent CT scan of the head was obtained in the emergency department, demonstrating a stable right frontal subdural hygroma and no new intracranial hemorrhage. Magnetic resonance imaging was then performed of the brain (See Figure 1).
Please click this link for diagnosis, workup, treatment and discussion.


