Thyroid eye disease, or Graves’ ophthalmopathy, is a potentially vision-threatening autoimmune disease that manifests most commonly in hyperthyroid patients (77 percent), and less frequently in euthyroid (20 percent) and hypothyroid (3 percent) patients.1 TED can precede or succeed the thyroid disease, usually within 18 months of each other in the majority of the patients.2 Although great variability in severity and duration of the disease can be observed, TED is ultimately a self-limiting disease that lasts about one year in non-smokers and three years in smokers.
Risk Factors
TED occurs between the 3rd and 6th decades, at a rate of 16 women and three men per 100,000.2 Although it is more common in women, men tend to exhibit more severe disease and present at a more advanced age. Cigarette smoking is the strongest modifiable risk factor resulting in more severe disease, which is less responsive to immunosuppressive therapy. Additionally, use of radioactive iodine (RAI) for hyperthyroidism has been associated with the development or worsening of TED. However, this has become more controversial as evidence suggests that rapid stabilization of the thyroid hormones after RAI treatment can prevent adverse progression. Genetic factors appear to play a role in TED, but specific contributions have yet to be elucidated.4,5
Pathogenesis
The pathogenesis of TED is incompletely understood, but is believed to be due to a reaction of T lymphocytes with antigens present in both the thyroid gland and the orbit. This reaction initiates a cascade of events that lead to the release of cytokines and other inflammatory mediators, resulting in proliferation of orbital fibroblasts, expansion of adipose tissue and enlargement of extraocular muscles. This inflammatory increase in the periorbital and orbital structures is responsible for the clinical manifestations of TED.6
Clinical Features
In general, approximately 30 to 50 percent of patients with thyroid disease have ophthalmic manifestations, of which only 3 to 5 percent of the patients constitute the vision-threatening spectrum of the disease.7 Patients will commonly present with complaints of diplopia, changes in the appearance of their eyes or symptoms related to corneal exposure, such as foreign body sensation, photophobia, redness and tearing. Patients will also complain of eyelid fullness or swelling and present for an evaluation for a blepharoplasty, which of course should be avoided during the active phase.
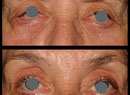
The most common and specific clinical finding for TED is eyelid retraction, occurring in about 91 percent of the patients (See Figure 1a). This is followed by proptosis (62 percent); motility dysfunction (43 percent); pain (30 percent); epiphora (23 percent); and compressive optic neuropathy (6 percent).8 Hence, in the clinical setting, it is important to measure the degree of inferior and superior scleral show, exophthalmos and motility. Oftentimes, patients will complain of soreness or a “pulling” sensation during the motility exam, especially in upgaze. The degree of lagophthalmos should be noted, and is often helpful to correlate with conjunctival and corneal changes. Chemosis is an extremely common finding, while corneal changes could range from mild punctate epithelial erosions to ulcerations and stromal thinning, usually along the inferior half. Additionally, close attention must be paid to the pupil exam to assess for compressive optic neuropathy. Clinical signs are usually bilateral but can often be asymmetric or, less frequently, unilateral. Systemic signs can also aid in determining the status of their thyroid disease or even lead to the diagnosis of thyroid disease. These signs are often nonspecific and include fatigue, weakness, cold or heat intolerance, anorexia, skin or hair changes, changes in their sleep or appetite and mood instability.
These signs will often allow for a clinical diagnosis of TED, and also determine the phase of the disease. TED emerges in the active phase, where periorbital and orbital inflammation will lead to the manifestation of the ocular symptoms. This phase usually lasts about one to two years before it spontaneously remits. The active phase is then followed by a plateau phase, where symptoms generally stabilize or may show some improvement before entering the inactive phase. Maarten P. Mourits, MD, PhD, and colleagues described a Clinical Activity Score to aid in determining the phase of the disease (See Table 1).9 One point is assigned to each of the 10 listed symptoms or signs and a score of 3 or more indicates active disease. The phase of the disease will then ultimately determine the indicated workup and treatment.
Differential Diagnosis
Depending on the presenting symptoms, further workup can be necessary to rule out other possible diagnoses. For those patients presenting with signs of orbital inflammation or congestion, orbital cellulitis, idiopathic orbital inflammation (IOI), and other inflammatory conditions, such as sarcoidosis, should be considered. However, infectious causes are often linked to a history of a recent illness, especially sinusitis, or related systemic findings, such as a fever. Patients with IOI usually report a more acute onset, with pain being the most prominent symptom. A CT or an MRI can show an orbital abscess and/or sinus disease to clinch the diagnosis of an orbital cellulitis, while a tendon-involving enlargement of the extraocular muscles makes IOI a more likely etiology (See Figure 2). Sarcoidosis frequently reveals an enlarged lacrimal gland that necessitates a biopsy.
For unilateral cases, orbital tumors or traumatic causes such as carotid-cavernous fistula should be suspected given the right history. Although nonspecific, tumors can often show globe displacement, while a C-C fistula will exhibit classic signs, such as “corkscrew” vessels, a discernible bruit and pulsatile exophthalmos. Again, diagnostic imaging can confirm the diagnosis (See Figure 2). With primary signs of motility dysfunction, cranial nerve palsies, chronic progressive external ophthalmoplegia (CPEO), or myasthenia gravis should be ruled out as well. However, with these diagnoses, patients lack other classic TED findings, such as eyelid retraction, proptosis and orbital congestion. Additionally, CPEO and myasthenia gravis will frequently present with ptosis. It is important to keep in mind, though, that myasthenia gravis is significantly more likely in patients with thyroid disease.
Workup
A thorough history and a clinical exam are often adequate to make a diagnosis of TED, and ancillary testing will assist in determining the clinical activity and severity of the disease. Visual field testing should be performed in patients with active TED, especially with concerns of compressive optic neuropathy. Findings are nonspecific, but can reveal enlarged blind spots, generalized constriction or paracentral or arcuate defects. CT or MRI will often show tendon-sparing fusiform enlargement of the extraocular muscles, with the inferior and medial rectus muscles being the most commonly involved (See Figure 1, B & C). Imaging will also evaluate for apical crowding to assess for compressive optic neuropathy. For those patients where the ocular symptoms precede the diagnosis of thyroid disease, it is important to obtain a thyroid panel. For atypical cases, a biopsy could be indicated.
Management
Once initiated, the eye disease functions and progresses independently of the thyroid disease, and thus should be managed independently. Stabilization of the thyroid levels should be achieved together with an endocrinologist. In the event that radioactive iodine is utilized to correct the thyroid disease, concurrent use of oral steroids tapered over a three-month period can prevent or minimize the effects on the eye disease.10 Modification of risk factors, especially smoking cessation should be strongly encouraged. Due to the self-limiting nature of the disease, observation or conservative therapy with lubrication is often sufficient for patients with minimal disease.
For patients in the active phase, the emphasis of treatment is decreasing or inactivating the inflammatory process and preserving vision. This is typically achieved with immunomodulation, radiotherapy and/or surgery. Oral corticosteroids (0.5 to 1mg/kg) tapered over a three to six month period, or in more severe cases, weekly IV steroids, have been utilized. Steroids prove especially useful in reducing pain, soft tissue improvement (i.e., eyelid edema and erythema), and temporizing optic nerve compression. Despite the benefits, the side-effect profile of corticosteroids prevents their long-term use. More side effects were noted with oral steroids including weight gain; hyperglycemia; hypertension; anxiety; mood lability; skin changes; gastrointestinal manifestations; and insomnia. For those who cannot tolerate the systemic effects of steroids, periorbital injections of steroids have been employed, but with less significant impact. Nonsteroidal immunomodulators, such as cyclosporine and rituximab, have emerged as alternatives. Thus far, their high cost, wavering efficacy and questionable side-effect profile have prevented them from being a first-line treatment.7,10,11,12
Although controversial, external beam radiation therapy, usually at very low doses (20 Gy), can be effective in achieving local control of active TED. Studies have shown radiotherapy to be the most useful in improving motility dysfunction. Development of cataract, radiation-induced retinopathy, optic neuropathy and secondary tumors are all concerns related to radiotherapy, but the risk remains low at the doses utilized for TED. Underlying diabetic retinopathy can potentiate the effects of radiation retinopathy, and thus is usually contraindicated for radiation. Greater benefit has been noted when steroids are used concurrently with radiotherapy.11,12
It is generally recommended that surgical intervention be postponed until the patient has entered the inactive phase or stabilization of his symptoms for at least three to six months. One exception is when the vision is threatened from compressive optic neuropathy or severe proptosis with resultant corneal ulceration or stretch optic neuropathy. In this instance, orbital decompression surgery is often employed as the first-line therapy to preserve vision. In general, removal of one or two orbital walls and/or orbital fat is performed to decompress the optic nerve and allow the globe to retract. Once stability is achieved, strabismus surgery, if necessary, can then be performed, followed by eyelid surgery to correct the retraction as needed. Cosmetic surgery, such as a blepharoplasty, should be performed last and with caution.11
TED is a relatively uncommon orbital condition that requires a multidisciplinary approach to its diagnosis and management. Early recognition of the clinical activity and severity is crucial in determining the appropriate treatment that could ultimately result in preservation of vision.
REVIEW
Dr. Kim is an assistant professor of ophthalmology at the Emory Eye Center in Atlanta.
1. Wiersinga WM, Smit T, et al. Clinical presentation of Graves’ophthalmopathy. Ophthal Res 1989;21(2):73-82.
2. Wiersinga WM, Smit T, van der Gaag R, et al. Temporal relationship between onset of Graves’ ophthalmopathy and onset of thyroidal Graves’ disease. J Endocrinol Invest 1988;11:615-9.
3. Bartley GB. The epidemiologic characteristics and clinical course of ophthalmopathy associated with autoimmune thyroid disease in Olmsted County, Minnesota. Trans Am Ophthalmol Soc 1994;92:477-588.
4. Stan MN, Bahn RS. Risk factors for development or deterioration of Graves’ ophthalmopathy. Thyroid 2010;20(7):777-783.
5. Manso, PG, Furlanetto RO, Wolosker AMB, Paiva ER, et al. Prospective and controlled study of ophthalmopathy after radioiodine therapy for Graves’ hyperthyroidism. Thyroid 1998; 8(1):49-52.
6. Lehmann GM, Feldon SE, Smith TJ, Phipps RP. Immune mechanisms in thyroid eye disease. Thyroid 2008;18(9):959-965.
7. Bartalena L, Tanda ML. Graves’ ophthalmopathy. N Engl J Med 2009;360:994-1001.
8. Bartley GB, Fatrouechi V, Kadrmas EF, et al. Clinical features of Graves’ ophthalmopathy in an incidence cohort. Am J Ophthalmol 1996;121:284-90.
9. Mourits MP, Koornneef L, Wiersinga WM, Prummel MF, et al. Clinical criteria for the assessment of disease activity in Graves’ ophthalmopathy: A novel approach. Br J Ophthalmol 1989;73:639-644.
10. Gould DJ, Roth FS, Soparkar CNS. The diagnosis and treatment of thyroid-associated ophthalmopathy. Aesth Plast Surg 2012;36:638-648.
11. Stan MN, Garrity JA, Bahn RS. The evaluation and treatment of Graves’ ophthalmopathy. Med Clin N Am 2012;96:311-328.
12. Prummel MF, Mourits MP, Blank L, Berghout A, et al. Randomised double-blind trial of prednisone versus radiotherapy in Graves’ ophthalmopathy. Lancet 1993;342:949-54.
13. Kazim M, Garrity JA. Orbital radiation therapy for thyroid eye disease. J Neuro-ophthalmol 2012;32:172-176.