In some ways, selecting an intraocular lens for cataract surgery is like jumping into a lake before you know its depth—and you never really know for sure until you break the surface, or, in the case of surgery, until the lens is in position postoperatively. Several companies and researchers, though, are working on ways to help surgeons home in on the right lens power during the surgery itself—before they make the leap and choose a lens—in order to reduce the number of astigmatic or refractive surprises postop. Here, cataract surgeons and intraoperative aberrometry developers explain the current state of the art, as well as how you can get the best results if and when you decide to use such a system.
WaveTec Vision’s ORA
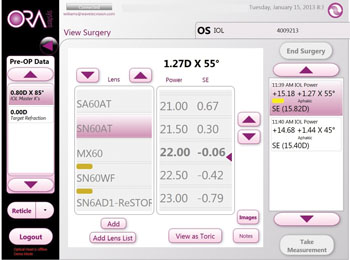
The Optiwave Refractive Analysis system is the only intraoperative aberrometer available for sale in the United States. The device attaches to the operating microscope and can be used for aphakic refractive measurements to help choose the proper lens, and for pseudophakic measurements to help rotate toric IOLs to the proper axis as well as to view the effect of limbal relaxing incisions as they’re created, giving the surgeon a chance to enhance the cuts for greater effect.
|
Several years of experience with WaveTec’s systems, starting with the original ORange, have taught surgeons certain techniques to make the most of the measurements.
“You want to make sure the cul-de-sac is clear and the lid speculum isn’t pressing on the lid or orbit,” explains Venice, Fla., ophthalmologist P. Dee Stephenson. “You want to ensure the cornea is moist and clear, the pressure is stable and that the patient isn’t looking down, but is instead looking superiorly.” Surgeons also say topical anesthesia is a must because they need the patient to stare at a fixation light during the measurement. “You also want the microscope position fairly coaxial, so there isn’t much tilt of the scope and it’s aligned perpendicular to the patient’s eye,” says Dr. Weinstock.
To proceed with the aphakic reading after the cataract has been removed, Dr. Weinstock first uniformly fills the eye with cohesive viscoelastic. “When I see the viscoelastic start to prolapse out of the wounds, it means I’ve filled the entire capsule and anterior chamber with it,” he notes. “I then seal the globe and check the pressure to make sure it’s between 18 and 30 mmHg. That’s when I know I’m going to get a good reading. There’s a camera image of the eye in which you can see the Purkinje reflexes, and a fringe-pattern image that gives a qualitative analysis of the quality of the tear film. If the tear film is irregular, the fringe pattern won’t look good or will be distorted. In these cases, you can sometimes squirt some more BSS on the cornea to improve the surface. With the patient fixating on the light, my assistant presses the touch screen to capture the image. It captures 40 images in five seconds or less, and then in 10 seconds or less it processes the information. It then displays the refraction and the suggested lens power. I compare that to what my preoperative lens selection was, based on preop biometry. I will also look at the preop cylinder versus that which was measured and use that as a guide to how accurate the readings are.
“Every patient is brought into the OR with four or five IOLs, usually 1 or 2 D above and 1 or 2 D below the IOL power we selected preoperatively,” Dr. Weinstock adds. “For a post-LASIK patient, we bring him in with IOLs up to 3 or 4 D above and below the projected power. No patient has the lens package opened until the intraoperative biometry is done, the data’s analyzed and compared to the preop data, and a final decision is made. Then the lens is opened and placed on the table.” Dr. Weinstock says in many cases the actual power needed as identified by ORA is more than 0.5 D different from the preop one that was identified, and can be off by 2 D or more in someone who has had previous refractive surgery.
An aphakic measurement also helps with limbal relaxing incisions, surgeons say. “When you remove the cataract, there might be more or less astigmatism than expected,” explains Dr. Stephenson. “The beauty of using ORA is, once the patient is aphakic, you do a measurement and you know how much astigmatism the cornea itself has. You can then titrate the amount of correction with an incision. For example, if you decided you were going to do two LRIs with 30-degree arcs at 600 microns and the ORA reading tells you that the astigmatism is reduced, that’s great. But if it’s not, you can enhance the incision—and always go deeper before you go longer.”
Dr. Stephenson says there are functions to help manage astigmatism with lenses, as well. “With a toric implant, the ORA readings show the amount of astigmatism, what you could expect to correct, the axis, and how much astigmatism would remain if you were to implant a certain lens power,” she says.
Surgeons say there are times when the measurements will make them take a step back and evaluate things before proceeding. “There’s some thought that goes into it, it’s not a device for which you just accept the reading at face value,” says Dr. Weinstock. “It’s no different than doing an IOLMaster and comparing that measurement to the Lenstar, or doing a Lenstar and comparing it to immersion. It’s another data point to use in decision making. Sometimes, you’ll get a reading that is way off, where the IOLMaster and immersion say one thing, but the ORA is, say, 3 D different. If this happens, I’ll go back and make sure the speculum isn’t pushing down on the globe, or that there’s not a dry area on the cornea, and then repeat the measurement. However, some eyes are just unusual. RK eyes are very sensitive to changes in IOP, and their corneas can have really unusual shapes. Actually, RK eyes are the ones I find to be least reliable on the ORA. There have also been readings that don’t make sense altogether and it turned out that, for one reason or another, we didn’t identify that the patient had previous LASIK—but the ORA identified it intraoperatively.”
Dr. Weinstock recalls one case where there was a significant difference between the ORA reading and the preop biometry. “In a patient who had had previous myopic LASIK, the ORA said 21 D for the power but the two other measurements that we did preoperatively, the IOLMaster and immersion, both recommended an 18-D lens,” he says. “So I went back and looked at the preop data, what K values were used for that, and it turned out we used the IOLMaster Ks for the IOLMaster reading and the manual Ks for the immersion. When I looked at the Ks from the Nidek OPD, they were much flatter than the ones we used in those formulas, so it led me to believe that our manual and IOLMaster Ks weren’t accurate. Looking at the patient’s history, she was a -6, but there was only a 4-D change on the keratometry based on these readings, except for the Nidek OPD. It turns out that the real Ks were much flatter than the ones measured preoperatively, and we would have been 2 to 3 D off if we didn’t use the ORA.”
To help increase the accuracy of its calculations, the ORA employs a feature called the WaveTec AnalyzOR, which accumulates the data from all ORA users in an effort to hone the system’s lens calculations. “Part of this is analysis software that let’s you track your own outcomes, to see how close you are to your targets, how you’re doing, and to develop your own personal nomogram in ORA,” says Dr. Weinstock. “The machine is also connected to WaveTec, and they take the global data and, based on that, they perform software updates to each unit that will change some of its proprietary formulas and surgeon factors both individually and globally. The company will get an overall look at the outcomes for all users using a particular lens, for example, and it can adjust its formulas based on that data in order to refine them.”
In terms of its use in their practices, Drs. Weinstock and Stephenson don’t use ORA on everyone, just on patients who have upgraded to a premium surgical package, for whom it’s an extra charge. “It’s improved my outcomes,” says Dr. Weinstock. “Our numbers show that, about 60 percent of the time, the ORA results in my using a lens power that’s different from what I would have selected based on preop measurements. Even though in many cases I’m only changing the lens power by 0.25 or 0.5 D, it’s dialing me in that much closer.” Dr. Stephenson says she’s tracked her improvement with different lenses. “Using ORA when implanting certain lenses has improved my accuracy. For instance, in my practice, with the Akreos lens, 92 percent of patients are within 0.5 D and 71 percent are within
0.25 D of the intended target. So, the results are as good if not better than LASIK’s. And with the new enVista lens, 96 percent of my patients are within 0.5 D and 73 percent are within 0.25 D. By entering my postops in WaveTec’s AnalyzOR, I’ve been able to personalize my surgeon factor and optimize my outcomes. I follow my outcomes closely and have raised the bar for my practice.
“For me, intraoperative aberrometry is a must,” Dr. Stephenson continues. “Patients today, especially baby boomers, want perfection, and ORA gives me the confidence to know I am giving my patients the best visual outcomes.”
Products in the Pipeline
On the horizon, there are a couple of groups working on new devices, each with its own approach to intraoperative aberrometry.
Clarity Medical Systems’ HOLOS IntraOp is a system designed to be mounted on the surgical microscope and used to produce continuous refractive data.
David Chang, MD, clinical professor at the University of California, San Francisco, has worked with Clarity on the HOLOS, and explains the device’s unique approach. “Current clinical wavefront measuring devices are based on Hartmann-Shack or Talbot-Moiré technology—which were originally developed for astronomy,” he says. “HOLOS incorporates an entirely new wavefront measuring technology that was specifically developed for the optical axis of the eye. This optimization shortens the time for data acquisition and analysis to an enormous degree. The result is that data can be continuously measured and displayed in real time. Comparing HOLOS to its predecessors is a bit like comparing a still camera to a video camera.”
What the surgeon sees during the operation will be “akin to a real-time refractive movie,” says Barry Linder, MD, Clarity Medical Systems’ chief medical officer. “He or she will be getting the sphere, cylinder and axis continuously. The surgery can also be reviewed post-surgery, with the system’s DVR capability. A higher-order aberration display won’t be part of the initial product, but is a capability of the HOLOS technology platform.”
|

In terms of availability of the device, it’s possible that U.S. surgeons will have a commercial model some time this year. “Clarity Medical Systems’ current plan is to have HOLOS IntraOp ready for limited release in the United States by the end of 2013,” Dr. Linder says.
Another potential system for intraoperative aberrometry is the Aston Aberrometer, which is in the prototype testing phase at Solihull Hospital and Aston University in Birmingham, United Kingdom. The system uses the Hartmann-Shack principle to return measurements in real time, and its designers say it’s designed to be attached to a slit lamp or under the surgical microscope coaxial with the surgeon’s line of sight.
Uday Bhatt, MD, an ophthalmologist taking part in the device’s development, says it has a dioptric range of around 45 D, and can measure aberrations up to the sixth order. “Measurement depends on which part of the reading you want to focus on—higher or lower,” he says. “The lower order will give you the refraction and spherical aberration as well as toricity. We haven’t done much work on the toric as of yet. At some point, though, we will go through the study protocol to perform a study of its use with toric lenses, as well.”
In a recent study of the device, Dr. Bhatt and his colleagues attached the aberrometer to a modified slit lamp base and used it to record refractive error and higher-order aberrations in 75 subjects. They compared the findings to those from an existing aberrometer, the Topcon KR1W. In a proof of concept, they found the Aston’s measurements to be similar to the Topcon’s.1
The next step is to look into intraoperative use. “Right now, we’re looking at whether we can actually use it intraoperatively and measure the refractive error of the aphakic eye,” says Dr. Bhatt. “That’s the potential we feel it has.” REVIEW
Drs. Weinstock and Stephenson are consultants to WaveTec. Dr. Chang is a consultant to Clarity Medical Systems.
1. Bhatt U, Sheppard A, Shah S, et al. Design and validity of a miniaturized open-field aberrometer. J Cataract Refract Surg 2013;39:36-40.




