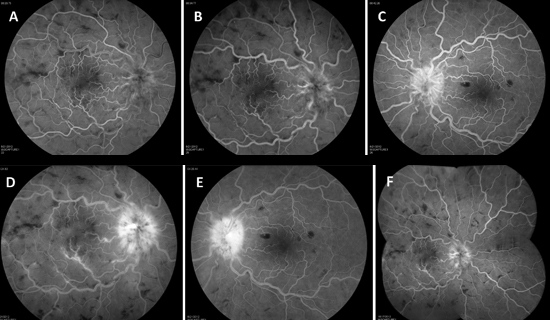
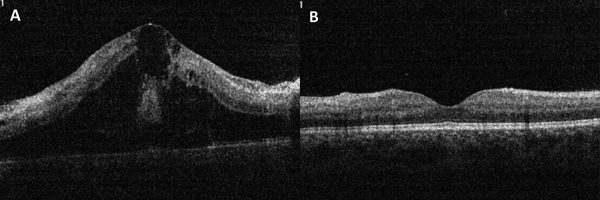
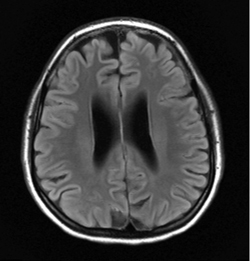
The patient underwent further imaging to characterize the retinal pathology. Fluorescein angiography showed hyperfluorescence of the disc and retinal veins consistent with leakage and staining (See Figure 2). Optical coherence tomography demonstrated significant macular edema in the right eye and a normal macula in the left eye (See Figure 3). The patient was admitted to the internal medicine service at Thomas Jefferson University Hospital for a comprehensive systemic workup including Infectious Disease and Rheumatology consults as well as neuroimaging. She was empirically started on IV ceftriaxone. A brain MRI showed scattered subarachnoid hemorrhages in the bifrontal region with subtle, likely reactive, leptomeningeal enhancement, bilateral optic disc prominence and enhancement and normal optic nerves (See Figure 4). A stat Neurology consult was obtained, deep vein thrombosis prophylaxis was discontinued, and empiric acyclovir and methylprednisolone 1 gram IV daily were initiated.
|
Given the patient’s history, exam and risk factors, a broad workup was initiated to rule out human immunodeficiency virus; tuberculosis; Lyme disease; syphilis; cat scratch disease; toxoplasmosis; human herpes virus 6; cytomegalovirus; Epstein-Barr virus; west Nile virus; Rickettsia panel; ehrlichia and anaplasmosis; sarcoidosis; rheumatoid arthritis; systemic lupus erythematosus; antiphospholipid antibody syndrome; small vessel vasculitides such as Wegener’s granulomatosis; and blood and urine cultures.
Throughout her hospital stay the patient remained asymptomatic except for her decreased vision. MRA imaging ruled out aneurysm and CNS vasculitis. Her workup was notable for Lyme studies that showed IgG reactive, and 1 of 3 IgM bands reactive, which was considered negative for re-infection. She was positive for Toxoplasma IgG but negative for IgM, ANA positive (1:40, homogenous staining), and her erythrocyte sedimentation rate was 45. All other investigations were normal. With negative viral studies, acyclovir was stopped.
Per Rheumatology, an associated auto-immune disorder was unlikely. Per Infectious Diseases, the patient’s workup was most consistent with aseptic meningitis. She received full pulse of three days of IV methylprednisolone followed by a tapering dose of oral prednisone. She was discharged on IV ceftriaxone to complete a 14-day course.
After two weeks her fundus exam showed significant improvement with less disc edema, less macular edema in the right eye, substantial decrease in perivenous sheathing, and resolution of the white-centered retinal hemorrhages peripherally. One month after presentation she was doing well with complete resolution of macular edema in her right eye. Her visual acuity improved to 20/100 in the right eye and 20/20 in the left eye.
|
Discussion
Frosted branch angiitis (FBA), or acute frosted retinal periphlebitis, is a rare clinical entity first described in the Japanese literature in 1976 in a 6-year-old child with idiopathic bilateral retinal periphlebitis.1 The severe sheathing of retinal vessels created the appearance of frosted tree branches. Fewer than 60 cases have been reported in the world literature, and the majority of cases (75 percent) are from Japan.2
The use of the term FBA in the literature as both a clinical syndrome as well as a clinical sign prompted Robert C. Kleiner, MD, et al, to distinguish three different subgroups based on their etiology.3 FBA can be classified as 1) primary idiopathic FBA; 2) secondary FBA due to infectious or auto-immune etiology; or 3) FBA in neoplastic processes.
The primary idiopathic form is the acute clinical syndrome comprised of young and otherwise healthy patients (10 to 30 years old) who typically present with bilateral visual loss and panuveitis.2,3 These patients typically respond promptly and favorably to corticosteroid treatment. The pathogenesis of this idiopathic variety is unknown, but hypothesized to be an immune-mediated mechanism directed towards an inciting antigen in the eye, possibly triggered by a bacterial or viral infection.2 Secondary FBA is associated with infectious diseases, including cytomegalovirus; tuberculosis; HIV, toxoplasmosis; Epstein-Barr virus; herpes simplex virus; varicella zoster virus; human T-lymphotropic virus; antistreptolysin-O; Coxsackie virus A10; adenovirus; measles and rubella; as well as with autoimmune diseases, including sarcoidosis; multiple sclerosis; lupus; Behçet’s, and Crohn’s disease.2,4,5 In this subgroup, FBA is a clinical sign of underlying disease as opposed to a distinct clinical entity. The pathogenesis for infectious etiologies is thought to be due to viral antigens forming immune-complexes and depositing in retinal vessels. Immune complexes are similarly responsible in autoimmune disorders.4 Frosted branch-like angiitis comprises patients affected by lymphoma and leukemia, in whom the pathology is thought to be caused by infiltration of retinal vessels with malignant cells.2
|
Our case is consistent with FBA due to aseptic meningitis. A letter to the editor of the European Journal of Neurology described a case of FBA associated with aseptic meningitis in 2000.8 This is the only other documented case of FBA associated with aseptic meningitis. Our case is unique, however, given the very prominent disc edema and scattered subarachnoid hemorrhages on presentation. Significant disc edema in the setting of FBA should prompt neuroimaging to rule out intracranial pathology. REVIEW
The author would like to thank Michael Dollin, MD, of the Retina Service for his time and assistance in preparing this case report.
1. Ito Y, Nakano M, Kyu N, Takeuchi M. Frosted branch angiitis in a child. J Clin Ophthalmol 1976;30:797-803.
2. Walker S, Iguchi A, and Jones NP. Frosted branch angiitis: A review. Eye 2004;18:527-533.
3. Kleiner RC. Frosted branch angiitis: Clinical syndrome or clinical sign? Retina 1997;17:370-1.
4. Quillen DA, Stathopoulos NA, Blankenship GW, Ferriss JA. Lupus associated frosted branch periphlebitis and exudative maculopathy. Retina 1997;17:449-451.
5. Rabb M, Jampol L, Fish R, Campo R, et al. Retinal Periphlebitis in Patients With Acquired Immunodeficiency Syndrome With Cytomegalovirus Retinitis Mimics Acute Frosted Retinal Periphlebitis. Arch Ophthalmol 1992;110:1257-1260.
6. Kleiner R, Kaplan H, Shakin J, Yannuzzi L, at al. Acute Frosted Retinal Periphlebitis. Am J Ophthalm 1988;106:27-34.
7. Watanabe Y, Takeda N, Adachi-Usami E. A case of frosted branch angiitis. Br J Ophthalmol 1987;71:553-558.
8. Johkura K, Hara A, Hattori T, Hasegawa O, Kuroiwa Y. Frosted branch angitis associated with aseptic meningitis. Eur J Neurol 2000;7:241.