With that in mind, four surgeons with extensive oculoplastic experience share their thoughts on which oculoplastic issues are most likely to impact cataract surgery, and what a surgeon should do when they arise.
Upper Eyelid Concerns
Generally, ptosis doesn’t increase the risk of cataract surgery; in fact, there is some argument for waiting until after the cataract surgery to deal with it. However, in severe cases it may need to be repaired first.
Jonathan Dutton, MD, PhD, FACS, professor and vice chair of ophthalmology at the University of North Carolina at Chapel Hill, notes that if ptosis is mild and primarily a cosmetic issue, most cataract surgeons won’t choose to do anything about it. “However, many patients who are going to have cataract surgery are sent to me to bring the lid up because it’s so low that it’s blocking their vision,” he says. “Doing cataract surgery will have limited benefit if your lid is still in the way of your vision afterwards. So if the patient has significant ptosis, it probably ought to be fixed before the cataract surgery.”
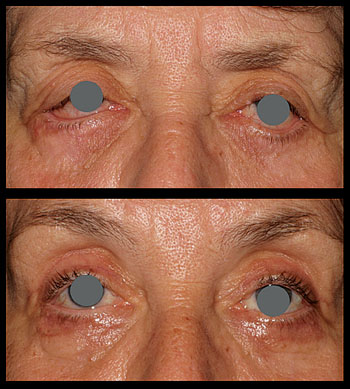
Julie Ann Woodward, MD, associate professor of ophthalmology and dermatology and chief of the Oculoplastic and Reconstructive Surgery Service at Duke University School of Medicine in Durham, N.C., notes another issue of concern. “A patient may have dermatochalasis, where the redundant upper eyelid skin is heavy and lying on top of the eyelashes,” she says. “This can create conditions favorable for blepharitis because there’s a warm, sticky environment that’s conducive to bacterial growth underneath the flap of skin.
|
One factor that needs to be considered before correcting ptosis is the patient’s dry-eye status. “If a surgeon refers a patient to us for ptosis repair and the patient has very dry eye, sometimes we’ll recommend either no ptosis surgery at all or a very conservative ptosis repair,” says Dr. Woodward. “We’ll explain to the patient that we can only lift the eyelid 1 or 1.5 mm to avoid worsening the dry eye. The more we correct the ptosis in this situation, the worse the patient’s dry eye will become.”
Dr. Dutton concurs. “The more you open the palpebral fissure by correcting the ptosis, the more dryness the patient will have,” he says. “That’s why some oculoplastic surgeons do a Schirmer’s test on every patient over 40 or 50. It’s not a great test, but it gives you some idea of tear function. In any case, if I see a patient with any kind of dry-eye issue and I’m planning ptosis surgery, I’m very conservative. I’ll lift the lid up just enough to clear the pupil so the patient can see. You don’t want to make these patients bright-eyed and bushy-tailed the way you might a younger patient, because you could be throwing the patient into a much more symptomatic dry-eye situation.”
Making the Droop Worse
“One thing I see all the time—and this is fairly well-documented—is upper lid ptosis a month or two, sometimes a year after the cataract surgery,” notes Dr. Dutton. “In the literature there have been debates about whether the cataract surgery is responsible for the ptosis; the consensus is that it probably is. During cataract surgery you put a speculum in and rotate the eye down to get at the superior limbus. There are adhesions between the superior rectus and the levator muscle in the orbit; when you pull one of them in one direction and the other in the other direction, you can theoretically damage those adhesions, causing ptosis. Because of the nature of cataract surgery, there’s not a lot we can do to prevent it.”
|

“In any case, if a patient comes in for cataract surgery with a few millimeters of ptosis, I wouldn’t repair it until after the cataract is done,” he says. “If you fix it to make the lids equal, the patient could develop a little droop again after the cataract surgery, requiring a second ptosis surgery.”
Dr. Woodward agrees. “Cataract surgery has about a 1-percent chance of worsening eyelid ptosis,” she says. “If patients need ptosis surgery, we usually recommend that they get their cataract surgery first. Of course, in some cases the ptosis is so severe that the surgeon finds it difficult to make certain measurements. In those cases we may go ahead and do the ptosis surgery first.”
Lower Lids and Exposure
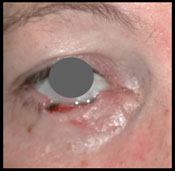
“Another issue to think about is lower lid ectropion, where the lower eyelid is very lax and the patient has sclera showing between the cornea and lower lid margin,” says Dr. Woodward. “Patients with this issue can be more prone to exposure-related dry eye and infections. If there’s a lot of sclera showing inferiorly, the cataract surgeon may suggest having the lower lid tightened so it better approximates the lower edge of the cornea prior to surgery. Normally, the lower eyelid should touch the inferior edge of the cornea or limbus and the upper eyelid should cover about 2 mm of the superior cornea.
“Ectropion is very common,” she adds, “especially in cases of sleep apnea. Patients with sleep apnea tend to have floppy eyelids along with their floppy palette. They are also more likely to be eye-rubbers and have a lot of mucus in the eyes; the eyelids can flip inside-out on the pillow. Such patients should be referred to oculoplastic surgeons for lid tightening prior to any cataract surgery.”
“If you’re doing cataract surgery on a patient who has any difficulty closing his eyes, or has exposure symptoms, that should probably be addressed before the cataract surgery,” agrees Dr. Massry. “Unlike ptosis, ectropion and entropion predispose the patient to irritation and infections after surgery. Furthermore, the individual may be asymptomatic and complication-free before surgery but start to have problems with dry eye or scratchiness afterwards. You never know how surgery will change the balance in the eye. So it’s worth addressing this beforehand, in part because any exposure may increase the risk associated with cataract surgery, but also because you don’t want the patient to blame related postop problems on the cataract surgery.”
Too Many Tears
“Anyone with excessive tearing should probably have that addressed before cataract surgery,” says Dr. Massry. “When tears well up and sit on the eye, it’s like water in a bathtub; after a while the tears can become murky and infected. If you’re doing cataract surgery, that’s the last thing you want.”
John S. Jarstad, MD, medical director of Evergreen Eye Centers in Federal Way, Wash., and an adjunct professor at Pacific Northwest University College of Osteopathic Medicine, in Yakima, Wash., agrees that addressing issues such as a blocked tear duct with excessive eye watering prior to cataract surgery is crucial. (Dr. Jarstad does numerous cataract surgeries every week, but has also done thousands of oculoplastic procedures over the course of his career and continues to do them whenever circumstances permit.) “A blocked tear duct is a setup for infection,” he notes. “In those cases, we’d like to see a dacryocystorhinostomy performed or tubes placed into the tear ducts to allow adequate drainage.”
“Patients’ eyes can tear for a number of different reasons,” notes Dr. Woodward. “First, the eye can water because it’s inherently dry. The dryness could be the result of not making proper mucus or oils for the hydrophobic layers that lie above and below the aqueous layer in the tear film; the eye tries to protect itself by reflexively producing extra aqueous fluid from the lacrimal gland.
“A second reason eyes can water is malposition of the punctum, which can happen with an ectropion,” she continues. “An ectropion can be repaired using a number of different approaches. If the problem is just lid laxity, a tarsal strip can be performed; if the punctum itself is everted, we may perform a medial spindle operation. Sometimes a skin graft is needed to reposition the puncta.
“The third reason an eye can water is blockage in the nasolacrimal duct,” she says. “If fluid doesn’t flow freely through the nose, bacteria may sit in a stagnant area and then flow retrograde back out onto the eye, potentially contaminating the cataract wound. For that reason, if the patient has an eye-watering issue, he needs to be evaluated to make sure there’s no nasolacrimal duct obstruction, especially if there’s any evidence that the patient may have had dacryocystitis in the past. If there is a problem, we might resolve it either by inserting a Crawford tube or by performing a dacryocystorhinostomy.”
In terms of deciding when tearing is sufficient to warrant intervention, Dr. Jarstad says the medical history is a big part of the answer. “Also, I ask the patient, ‘Do you have tears running down your cheek?’ If they say yes, I’m concerned,” he says. “I also examine the tear film, staining the eye with vital dyes like rose bengal or lissamine green, and do fluorescein testing.”
Additional Concerns
Cataract surgeons may encounter other issues as well:
• Tumors. “I see a lot of malignancies involving the eyelids,” says Dr. Dutton. “They’ve often been misdiagnosed as inflammation or blepharitis. Blepharitis doesn’t occur in one location, on one lid, but general practitioners sometimes make that mistake. Would an incorrectly diagnosed malignant tumor affect cataract surgery? The cataract surgeon is putting in a speculum and rubbing all over the lids; I don’t know whether that could dislodge tumor cells.
“I think any ophthalmologist who sees a lesion on the lid should question the patient,” he continues. “How long has it been there? Does it bleed? Especially if it’s elevated, if it’s ulcerated, if there’s loss of lashes … those are all tip-offs that you may be dealing with a malignancy. Refer the patient to somebody who can make that diagnosis, if you can’t do it yourself.”
|

• Trichiasis. “If the eye is irritated because of the lashes coming back against the eye, the patient is going to have excess tearing,” notes Dr. Dutton. “I see a lot of these patients and their corneas are abraded, which is going to affect their visual acuity. If you take out the cataract but the cornea is in that condition, the patient isn’t going to be thrilled with the resulting vision. I think it makes sense to deal with this before proceeding with cataract surgery.
“One way to deal with this is to simply pluck out the offending lashes,” he notes. “Sometimes the lashes will grow back in the correct position, but in most cases they’ll grow back in the incorrect position, so this won’t be sufficient. We prefer to use a radio-frequency tool to remove the lashes permanently. I’d do this before the cataract surgery.”
When Should You Refer?
Dr. Woodward notes that whether or not a cataract surgeon refers patients to a specialist for correction of oculoplastic concerns really depends on the comfort level of the surgeon. “Years ago, doctors were jacks-of-all-trades,” she says. “Many cataract surgeons felt comfortable taking care of ptosis and ectropion themselves. Today, ophthalmologists have become very subspecialized, and they’re more apt to refer patients to an oculoplastic specialist.
“However, this may depend partly on your location,” she adds. “In some cities, surgeons tend to stay subspecialized; in other cities, surgeons are more comfortable doing oculoplastic procedures themselves. Here at Duke University we have so many subspecialized ophthalmologists available that there’s no reason for surgeons to try to do these all of these oculoplastic procedures themselves.”
Dr. Massry agrees. “If you’re talking about an eyelid problem like an entropion, ectropion or ptosis, it’s all about the comfort zone and expertise of the physician,” he says. “Many ophthalmologists have been around for a while and are comfortable doing basic eyelid work. However, if you’re a surgeon who just does high-volume cataract all day, it may not make sense for you to do the eyelid surgery; your risk of having a complication is going to be greater than it would be for someone who does oculoplastic work all day. And plenty of specialists are available; 550 oculoplastic surgeons in this country are certified by the American Society of Ophthalmic Plastic and Reconstructive Surgery. It’s really up to the surgeon to decide.
“On the other hand,” he continues, “if the patient has tear duct blockage or a tumor, the surgery is a little more advanced and should probably be referred to a specialist. Ectropion, entropion and ptosis are bread-and-butter eyelid surgeries that many general ophthalmologists have been trained to do, and if the surgery doesn’t work out it can probably be corrected. That’s not the case with tumors or tear duct blockages, which most general ophthalmologists don’t treat routinely. In those cases, I would err on the side of being cautious and refer to an oculoplastic colleague.”
Strategies for Success
When examining a potential cataract patient, these suggestions can help avoid increased surgical risk:
• Don’t overlook the eyelids. “I think it’s important to pay attention to the ocular adnexa and look at the lid position,” says Dr. Jarstad. “It’s easy to overlook these. We’re usually very focused on looking at the eyeball, checking the cornea for corneal dystrophy, checking to make sure there’s no zonular weakness or pseudoexfoliation before we start, and checking the retina to make sure there won’t be any surprises due to macular degeneration or some other retinal disease. But we sometimes overlook the eyelids. In particular, significant laxity or a blockage in the nasolacrimal system really should be addressed before cataract surgery. Managing these concerns will give the patient a better outcome and lower the risk of infection or a prolonged recovery.”
Dr. Woodward agrees. “Of course, if a condition is severe, most cataract surgeons will notice it and address it, but sometimes they overlook it if it’s mild,” she says. “As a result, patients don’t get treated for dermatochalasis, ectropion or ptosis, even when the patient might benefit and the cataract surgery would be safer.”
“Cataract surgeons can get so busy looking at the cataract that they forget the lids, conjunctiva, tear ducts and so forth,” says Dr. Dutton. “For example, I’d say that 40 to 50 percent of the patients I see who have skin cancer aren’t even aware of it. Somebody has to point it out to them; they just thought the lesion was a little sore or something and paid no attention to it. The cataract surgeon is in a position to find those things at the initial examination.
| ||||

• Don’t assume oculoplastic issues can be addressed after the cataract surgery. “I think there’s a tendency to assume you can take care of these issues after cataract surgery, because that’s how many plastics problems are addressed,” says Dr. Jarstad. “Some issues like ptosis can be affected by the cataract surgery, so it makes sense to address those later. But other issues really need to be addressed before the cataract surgery to avoid putting the patient at risk.”
• Alert a patient of existing ptosis. “If a patient of yours is going to have cataract surgery and already has a droopy lid, you need to point this out beforehand so the patient doesn’t blame it on your surgery,” says Dr. Massry.
• If the upper eyelashes point straight down, ask the spouse whether the patient snores. “Upper eyelid lash ptosis is one of the signs of floppy eyelid syndrome,” Dr. Woodward explains. “Floppy eyelid syndrome is on the spectrum of floppy palate, and these individuals frequently have sleep apnea. So if you observe that the lashes point straight down, it’s important to ask the patient and even the spouse whether the patient snores. The spouse will often say, ‘Yes, like a freight train,’ or, ‘Yes, he has a CPAP machine.’ Sometimes the patient is already being treated for sleep apnea, but sometimes patients haven’t been treated before. In that case it’s really important for us to refer them for sleep studies, because treating sleep apnea can potentially prolong the patient’s life.”
• If appropriate, try the snap-back test. “Occasionally you’ll encounter a patient with involutional ectropion, where the eyelids are very lax and don’t approximate the globe well,” notes Dr. Jarstad. “Those patients are at risk for exposure and infection after surgery. In that situation I was taught to do the snap-back test, where you pinch the lower eyelid and pull it away from the globe and let it spring back. If it takes more than a second or two to spring back and approximate the eyeball, the patient may require some eyelid tightening with a tarsal strip procedure or a wedge resection before surgery.”
• If the patient is tearing excessively, determine the cause. “If the cause is mechanical, such as lid laxity or punctal stenosis, that shouldn’t affect the cataract surgery,” notes Dr. Dutton. “But if the tearing is due to blepharitis or a possible nasolacrimal duct infection, I’d get that fixed before cataract surgery. And if the patient is tearing but the cause isn’t obvious, you might want to refer the patient just to make sure that the lacrimal drain system is OK.”
• If something doesn’t seem quite right, don’t let it drop. Dr. Massry notes that sometimes a problem isn’t obvious, so it behooves the cataract surgeon to be alert for something that just doesn’t seem right. When that’s the case, he advises considering a referral.
“For example,” he says, “a general ophthalmologist referred a patient to me who had droopy, puffy lids. The patient said that the puffiness had been progressive, and was noticeably worse in one eye. When I examined him, I realized that a lot of the heaviness on the upper lid in the worse eye was not standard droopiness; the globe was a little more prominent and slightly inferiorly displaced. It was very subtle, but I ordered a CAT scan; it revealed a tumor in the orbit.
“There are several lessons worth noting here,” he continues. “First, if something doesn’t seem right, don’t let it drop. And if it potentially involves an area you don’t work with on a daily basis, refer to someone who manages those issues every day. When you work in a particular specialty for years, you learn to notice and identify subtle problems that would escape the notice of anyone else.
“Also, always take the patient at his word,” he adds. “If he has a complaint but you don’t find anything, assume he’s right; something is going on. Usually if you spend the time and search carefully, you’ll find the problem. If not, refer the patient. Don’t let it drop just because you can’t find the problem yourself.”
• If a patient refuses corrective surgery, inform the patient of the consequences and then reconsider. Dr. Massry notes that occasionally a patient won’t want to undergo the oculoplastic surgery. “Whether a corrective surgery is necessary for a given patient is always a judgment call on the part of the cataract surgeon,” he says. “If the surgeon feels that the problem is minor or inconsequential, or the patient’s a lot older and wouldn’t agree to go through the extra procedure anyway, then the surgeon has to decide whether or not it’s safe to do the cataract surgery given the patient’s condition. It’s really all about the judgment of the treating physician.
“For example, suppose a patient has had a little bit of ectropion for 20 years and doesn’t want to have surgery to fix it because he’s been doing fine,” he continues. “It’s possible that after you do the cataract surgery it will get worse and he won’t be ‘just fine’ any more. So you have to let the patient know that it could get worse.
“In this situation, all you can do is inform patients in an ethical manner,” he adds. “You can’t tell them what to do; they have to make their own decision. If they won’t agree to the extra surgery, then you have to decide whether you’re willing to proceed.”
Dr. Jarstad has encountered this as well. “I’ve had some patients who felt they could not endure a dacryocystorhinostomy, but they still want the cataract surgery done,” he says. “That puts us in a little bit of a bind because we have to make sure that they’re not at risk of infection. In this situation we treat them with antibiotic eye drops for a couple of weeks before surgery and then go ahead. In our experience that has worked, but it’s definitely more risky. We’ve had to do this several times in the past 27 years, and so far we have not seen infections or other issues.”
• Don’t be afraid to refer. “The majority of patients we see are great candidates for cataract surgery,” notes Dr. Jarstad. “But nowadays almost everyone has the option of referring a patient to an oculoplastic specialist or someone with experience in oculoplastics. If you don’t feel you can deal with a problem, I wouldn’t hesitate to refer the patient.”
How Much Risk is Acceptable?
Undoubtedly, many cataract patients who might have benefitted from having oculoplastic issues addressed before cataract surgery have not, either because the condition went unnoticed, or because the surgeon felt that addressing the problem wasn’t necessary. In most cases, the patients probably didn’t suffer any vision loss as a result.
Nevertheless, whether proceeding in a borderline situation is ideal is open to question. “If I were doing cataract surgery, I wouldn’t want to take any risk whatsoever, no matter how small,” says Dr. Dutton. “I’d get everything about the eye in good shape before doing the surgery. There’s no reason to do cataract surgery if the patient is going to complain afterwards that he can’t see or that his eye hurts all the time.
“Patients are always going to blame you if they have any problems after you’ve done surgery on them, whether the problem was there beforehand or not,” he adds. “So, you might as well take care of those issues first.” REVIEW


