As cataract surgeons know, their surgery relies heavily on technique, but also on technology, especially intraocular lenses. On our latest survey of IOL preferences, many surgeons seem to be sticking to the lenses that provide the solid postop results they’re used to getting, but some are branching out into new options, such as premium lenses that have recently been approved in the United States.
This is just one of the findings from this year’s e-mail survey on IOL preferences. This time around, 25 percent of the 10,540 recipients on Review’s e-mail list opened the message, and 58 surgeons took the survey.
To read about your colleagues’ impressions and usage patterns of both the stalwarts and the new upstarts in the IOL arena, as well as their views on other intraocular lens technologies, read on.
 |
Premium Lens Options
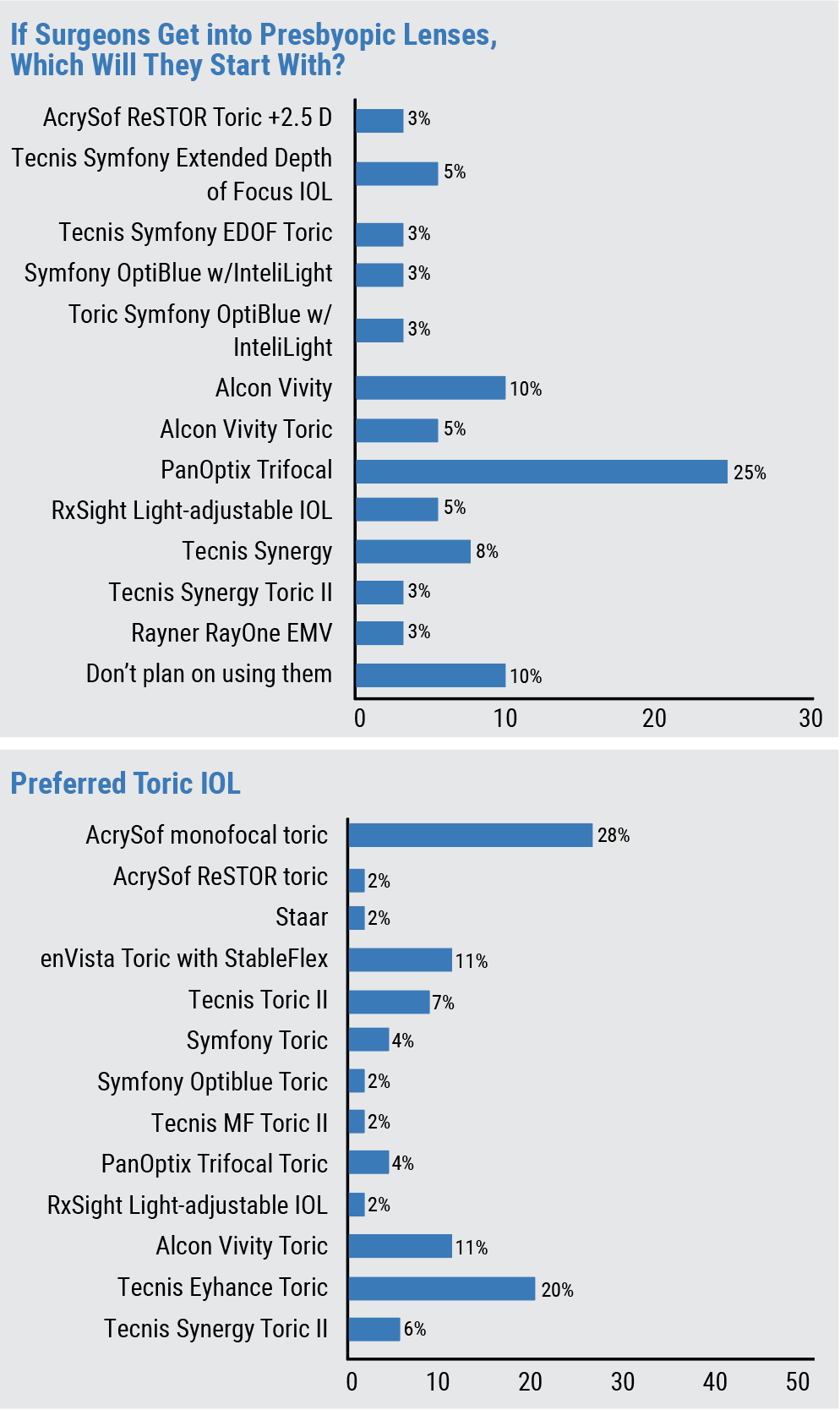
Surgeons on this year’s survey still seem to be leaning toward trifocal options, but newer additions to the premium intraocular lens marketplace are turning heads, as well.
The most popular premium lens on the survey (some surgeons chose more than one option) is the Alcon PanOptix Trifocal, used by 52 percent of the respondents. In terms of the average number of PanOptix lenses implanted per month, the users say they implant about eight lenses on average, at an average charge for the patient of $2,945 per lens. Next in line was the toric PanOptix, used by 47.9 percent of respondents (average number of PanOptix torics implanted per month: 7; average charge per lens: $3,172).
Paula Young, MD, of Alexandria, Virginia, says she implants the PanOptix but that there’s a bit of room for improvement in terms of “associated dysphotopsias and lengthy chair time.” A Kentucky surgeon also likes the PanOptix, but wishes it gave “a better range of vision,” he says, adding, “It still has unwanted halos.” A surgeon from Washington who primarily uses the PanOptix says he’s “somewhat satisfied” with the IOL, adding, “I dislike the reduced contrast sensitivity and the increased expectations from patients that come with the expense of the lens.” Jonathan Adler, MD, of Bradenton, Florida, likes the PanOptix, saying it “gives a great range of vision.” He notes, however, that it “needs to be implanted in eye without an epiretinal membrane, and not in post-refractive eyes.”
 |
Next in line is the Alcon Vivity IOL, used by 39.6 percent of respondents (average number implanted per month: 6; average charge per lens: $3,164). Close behind is the Vivity toric, used by 37.5 percent of the surgeons (average number implanted per month: 9; average charge per lens: $3,083). Dr. Adler says Vivity “gives excellent range of vision for post refractive patients.” Baltimore surgeon Ismail A. Shalaby says he likes the Vivity, but he would “love better near vision” from it.
Another popular lens was the Tecnis Synergy, used by 31.3 percent of respondents (average number implanted per month: 5; average charge per lens: $2,798).
Fifteen percent of the surgeons use the Rayner RayOne EMV IOL (average number implanted per month: 8; average charge: $1,748), and 10 percent implant the Crystalens (average number implanted per month: 1; average charge: $1,500).
In terms of the new offerings in the premium space, 19 percent of the surgeons use the Symfony OptiBlue with InteliLight (average number implanted per month: 4; average charge per lens: $2,924). The Lenstec Clearview 3 Multifocal is used by 13 percent of the respondents and 10 percent implant the new AcuFocus IC-8 Apthera (the surgeons choosing the Clearview and the Apthera didn’t provide data on lenses per month or how much they charge).
Toric IOLs
For tackling astigmatism, 28 percent of the surgeons say they use the AcrySof toric the most, followed by 20 percent who prefer the Tecnis Eyhance toric. Eleven percent of the surgeons use the Bausch + Lomb enVista Toric with StableFlex.
“It’s reliable, and easy to center and adjust,” says a surgeon from Washington about the AcrySof toric.
Bruce H. Cohen, MD, of St. Louis, prefers the Eyhance toric, saying, “It works well, with a broader range of focus and no glare.”
[The enVista Toric] IOL’s rotational stability is improved over lenses I previously used,” says a surgeon from Virginia.
The rest of the toric lens results appear in the graph above.
 |
Monofocal Mainstays
Surgeons also shared their thoughts on the bread-and-butter lenses for cataract surgery: the monofocals.
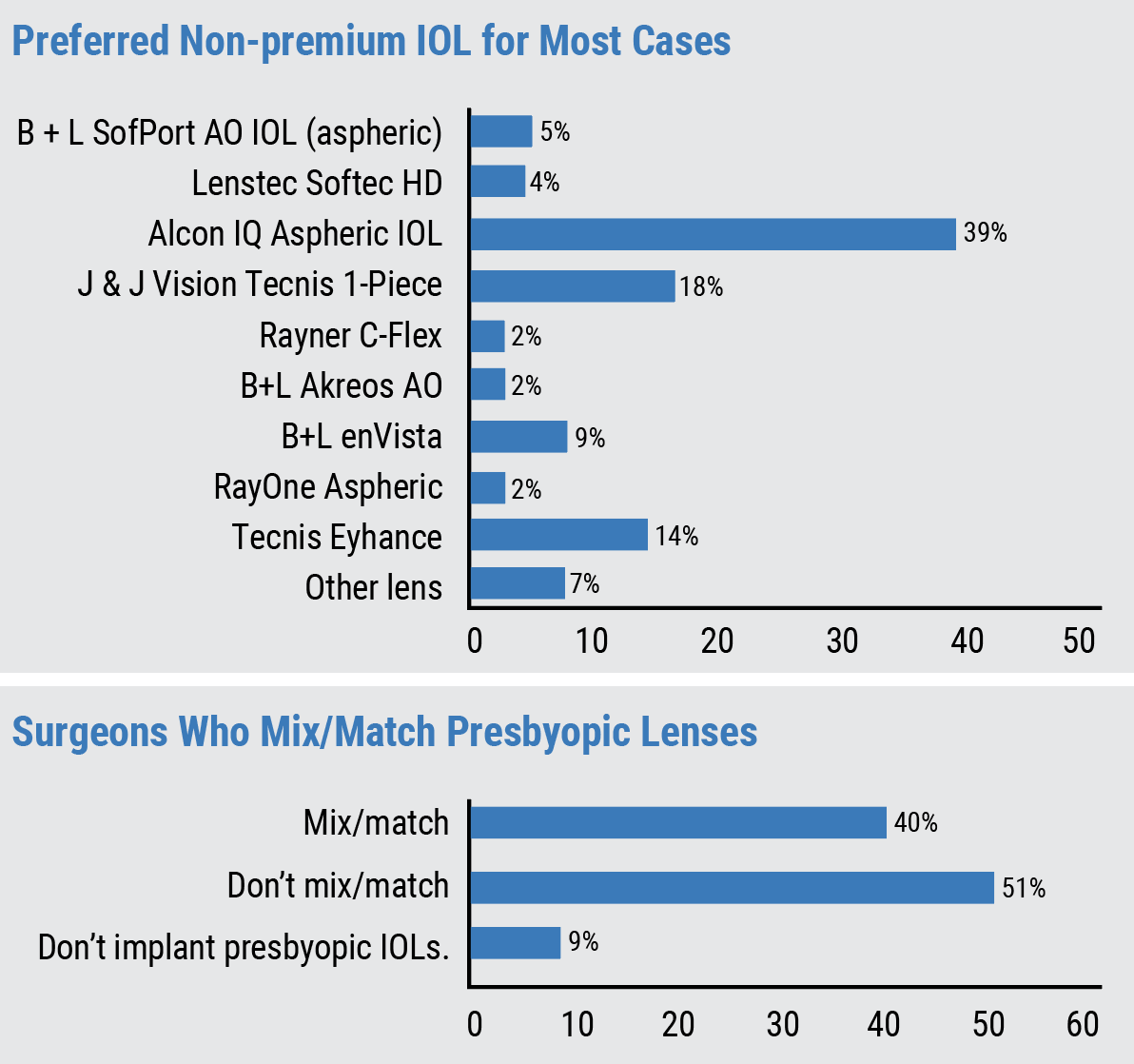
Thirty-one percent say they prefer the Alcon IQ Aspheric IOL, followed by the J&J Vision Tecnis One-piece (18 percent). The next most popular lens is the Tecnis Eyhance (14 percent), followed by the B+L enVista (9 percent).
A surgeon from Washington uses the AcrySof monofocal the most, saying, “I like that it is time-tested, easy to load and has delivered reliable outcomes for many years. I dislike that it is yellow-tinted.”
A doctor from Georgia prefers the Tecnis One-piece. “I like the clarity, color appreciation by patients, and lack of glistenings,” he says. A surgeon from California likes to use the Eyhance, noting, “[It’s part of the] Tecnis line: same A constant across the entire platform. It’s an easy-to-use, pre-loaded PCIOL.”
A surgeon in the enVista camp says he prefers it because it “opens cleanly, looks great on postop day one and there are no glistenings.”
All of the monofocal results appear in the first graph in this article.
Phakic Lenses
Only 28 percent of the respondents say they implant phakic IOLs. For those that do, all of them use the new EVO/EVO+ Visian (either the toric or non-toric version).
Manhattan surgeon Jimmy Hu says the EVO is a “great option for many patients, but it requires a lot of patient counseling.” He adds, “It’s also more involved surgery compared to LASIK/SMILE/PRK, and the patient needs to be aware of that. However, for high myopes, quality of vision is much better than LASIK/SMILE/PRK (because of fewer higher-order aberrations), and many of these patients are super happy.”
“They seem to be a niche technology that could be great for the right patient, but aren’t a first-line option for most patients,” says a doctor from Washington.
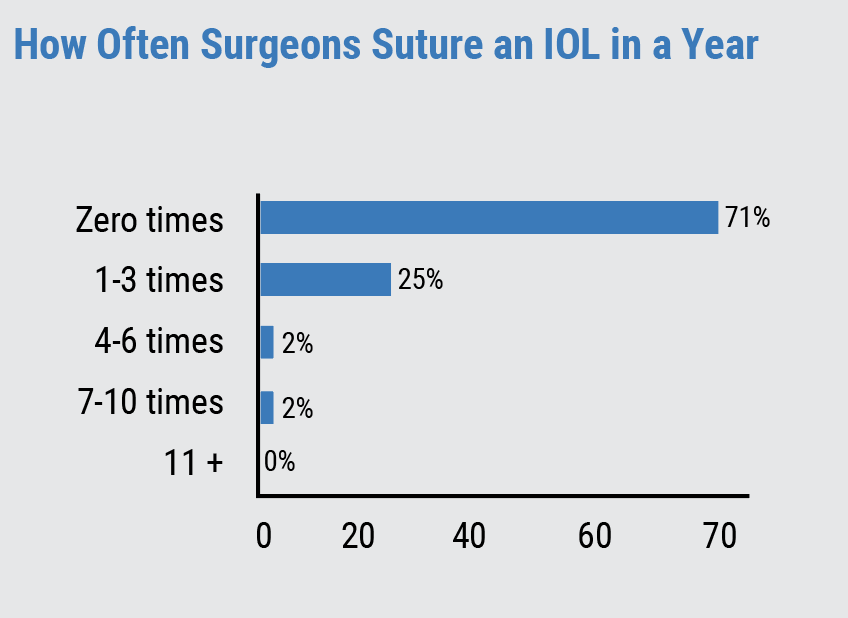 |
Suture Situations
For those rare situations in which there’s not enough support for an IOL in a patient’s eye, surgeons discussed their thoughts on suturing techniques. The frequency of having to suture a lens appears in the graph above.
A surgeon from North Carolina says in his experience, the usual causes for the instability are “floppy-iris syndrome and poor zonules.” A Pennsylvania surgeon cites “no bag support,” and adds that he scleral fixates.
“I don’t suture a lens to the iris, but I do perform scleral-fixated IOLs,” opines Dr. Hu. “I prefer either the Yamane technique using a Zeiss CT Lucia 602 lens, or Akreos AO60 fixation to the sclera with Gore-Tex sutures. I don’t perform iris fixation because even though it’s a technically easier surgery, the prolene sutures often break in about 10 years, requiring additional surgery.” A Texas surgeon agrees, saying, “I refer to retina, since scleral-sutured IOLs are better than iris-sutured lenses.”