Diagnosis and Presentation
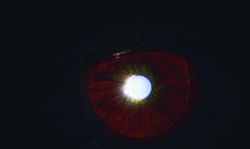
OCA is most often clinically diagnosed based on the features of ocular hypopigmentation (iris and retina), skin and hair, in conjunction with decreased visual acuity. Additional ocular signs include nystagmus; iris transillumination defects; foveal hyopoplasia; anomalous retinal vasculature; anomalous optic nerves; and an abnormal optic chiasm. One or two of these features may be absent, but decreased visual acuity is almost always a feature of this condition. It is important to remember that not all children with OCA will have the snow white hair and translucent irises that may first come to mind; there is a range of light blonde to brown hair and eye color can be blue, brown or hazel (See Figure 1). Therefore, albinism should be considered in the differential of any child who presents with chronic nystagmus and a fair complexion.
Nystagmus is almost always present,3 and is often the most bothersome and noticeable feature to the parents of children with OCA. The nystagmus typically develops over several weeks after birth. It starts as a large-amplitude, low-frequency pendular nystagmus, which parents sometimes interpret as an inability to fixate on objects.3 The nystagmus often dampens over time and may even disappear later in childhood.1 Stress, fatigue, illness and monocular occlusion all worsen nystagmus. Children may adopt head nodding and anomalous head positions in an effort to find a null point where the nystagmus is diminished. Visual acuity directly improves with decreased nystagmus. Clinicians should always make note of the patient’s binocular visual acuity (with preferred head position), as this will likely be significantly better than monocular acuity and reflects more accurately the patient’s visual function.
|

Macular hypoplasia is the most significant cause of decreased visual acuity in albinism. This is often evident on the fundus exam (See Figure 2). Spectral-domain optical coherence tomography is much faster than time-domain OCT, and can demonstrate the foveal hypoplasia and absence of the foveal pit, or “fovea plana,” which is characteristic of OCA, even in the presence of nystagmus.5 Other details demonstrated by SD-OCT include persistence of an abnormal, reflective nerve fiber layer band; persistence of multiple inner retinal layers; loss of the normal thickened photoreceptor nerve layer; and increased reflectivity of the choroid due to decreased pigmentation.6 RPE hypopigmentation has been shown to correlate with macular hypoplasia.3,10
In cases of significant foveal hypoplasia, the vasculature of the posterior pole becomes more anomalous, and vessels may be seen coursing near or through the area where the fovea should be. Besides foveal hypopigmentation and hypoplasia, there are also reduced numbers of photoreceptors—fewer rods in the macula and fewer cones in the foveal region.
Continuing posteriorly in the visual pathway, OCA patients also have anomalous optic nerves and optic chi-asm abnormalities, and the primary visual cortex shows disruption of binocular-driven neurons.
Best corrected visual acuity varies greatly among individuals with OCA. Most studies report a range of 20/30 to 20/400 with an average of 20/80.6 BCVA depends largely on the genotype and phenotype of the individual, as well as the vision care the patient receives throughout his or her life. The patient’s retinal image quality is degraded by refractive error (albinism patients are very rarely emmetropic), light scatter from the TIDs, and nystagmus, while the resolving power of the retina is limited by foveal hypoplasia.1 Children with OCA face significant ocular and optical hurdles while their visual pathways are still developing, and thus often develop amblyopia. Orthotropia is uncommon in albinism—they are often esotropic or exotropic, and their anomalous visual pathway anatomy precludes the development of high-grade stereoacuity.3
Pathophysiology
The mechanism of disease is deficient melanin production. This can be due to defective melanosome (the organelle in melanocytes which produces melanin) maturation, an abnormality of melanosome enzyme function, or a decrease in the number or distribution of melanocytes in the tissue.1 In the past albinism was characterized as tyrosinase-negative or tyrosinase-positive; however tyrosine production can be only partially affected, and there are other enzymes in the pathway that may be affected.
Genetics
The genetics of pigmentation is complex. More than 100 genes are involved in the pigmentation of the hair, skin and eyes. These genes are not expressed as simple Mendelian traits, but rather multiple genes are inherited and interact with each other, and this complex interaction generates a large range and variety of phenotypic expression. The albinism phenotype results from a defect in one or more of 13 genes that determine melanocyte function. These genes are inherited most often in an autosomal recessive fashion such as the tyrosinase gene on chromosome 11, protein P gene on chromosome 15, tyrosine-related protein gene (TRP1) on chromosome 11, and membrane-assosciated transport protein gene (MATP). But the most common form, accounting for 10 percent of albinism cases, is the X-linked GPR143 gene.3 All genotypes result in misrouting of the optic nerve fibers during embryogenesis and underdevelopment of the neurosensory retina, along with varying pigmentation of the hair, skin and irises. All races and sexes are affected.
Associated Syndromes
Hermansky-Pudlak Syndrome (HPS) is a rare condition globally, but occurs much more frequently in the northwestern and central regions of Puerto Rico, with an incidence of 1:1,800. It also occurs more fre-quently in the Swiss.3 It is important to be aware of this condition, which is associated with a potentially life-threatening bleeding diathesis caused by platelet storage pool deficiency. In addition to platelet aggregation defects, certain genotypes of HPS are also predisposed to interstitial lung disease, granulomatous colitis, and/or neutropenia. Patients with HPS often have visual acuities less than 20/200.2
All patients with the OCA phenotype who report any Puerto Rican or Swiss ancestry should be formally evaluated for HPS by their primary-care physician or hematologist. Testing for bleeding times and platelet aggregation is thought to be unreliable, and there are few commercially available genetic tests.2 On skin biopsy, abnormally large melanosomes, called macromelanosomes, are observed.3 HPS is suspected in baby boys with the OCA pheynotype who have bleeding complications after circumcision or in toddlers with excessive bruising.2 There are nine genotypic variants of HPS that have distinct phenotypes. Currently, commercial lab tests are available only for the HPS-1 and HPS-3 genotypes.
Chediak-Higashi syndrome (CHS) is a condition of OCA phenotype with associated neutropenia, natural killer cell dysfunction and frequent bacterial infections.2 CHS can also be associated with retinal dystrophy.1 The diagnosis of CHS in made by the presence of giant granules in neutrophils and other leukocytes. Griscelli syndrome is phenotypically similar to CHS, but lacks the giant granules.
Deafness may also be associated with albinism because of the affected pigmentation in the development of the stria vasculosa of the ear.3
Management
There is currently no cure for oculocutaneous albinism, but there are a number of measures that can be taken to improve your patient’s visual function and to educate him on the importance of protection from sun damage.
First and foremost, clinicians must aim to maximize correction of any refractive error. This can be difficult with the associated nystagmus, but it is important to do careful retinoscopy in young patients. Full correction of any myopia and astigmatism as well as any hyperopia greater than 2 diopters is recommended. Using tinted lenses to alleviate photophobia is helpful in some patients. Color filters have not been shown to objectively improve reading performance; however, there is significant subjective improvement reported. This improvement may be a placebo effect, but could also be due to the color filters improving asthenopia and photosensitivity through reduced chromatic aberration and contrast.7
Monitoring for strabismus and anomalous head positioning is important. The Kestenbaum-Anderson procedure can be utilized if a significant head-turn exists. This procedure involves large recessions and resections of all horizontal muscles, and parents should be cautioned about potential consecutive head turns and strabismus after surgery. Richard W. Hertle, MD, and colleagues found horizontal muscle tenotomy to be effective in dampening nystagmus and improving visual acuity.5 They have further shown patient quality of life surveys reflect this improvement; however, the power of their study was quite low (n=5 for patients with albinism).4 Parents should also be cautioned that the visual improvement will likely be limited by the degree of retinal hypoplasia.3
|
Skin and eye protection is of the utmost importance. Hypopigmented individuals are at increased risk of sunburn, photoaging and solar keratoses, as well as cutaneous malignancies: squamous cell carcinoma; basal cell carcinoma; and melanoma.2 Parents are advised to avoid sun exposure during peak hours; to wear wide-brimmed hats and UVA/UVB protective sunglasses; and to apply sunscreen with at least 30 SPF to all sun exposed skin, at all times. Vitamin D levels should be monitored because deficiency can result secondary to the necessary sun avoidance.
Children with albinism do not have cognitive delay and generally have normal to above-normal intelli-gence. They are often high achievers in school. As for infant and toddler motor skill development, they are typically within normal range or a couple of months behind their normally sighted counterparts. They do, however, have difficulty with fixation when reading.8 Relationships may be difficult during development because they may look very different from their schoolmates, and their visual impairment may lead them to get too close to people, which can be perceived as an invasion of personal space.1
As mandated by the Americans with Disabilities Act, an Individual Education Plan should be developed for each school-aged child with OCA and reevaluated annually.1 In addition, clinicians should consider a low vision referral to evaluate the need for magnifiers (near vision), handheld telescopes (distance vision), writing guides, closed circuit TVs and other devices such as bioptics. Bioptics are glasses with telescopes permanently mounted in them and may be used by some low-vision patients for driving.1
Genetic Testing/Gene Therapy
Genetic testing can help parents understand the basis and the risk of recurrence of OCA in future children. These tests can be quite costly and should be explained by a genetic counselor or ocular geneticist who is well-equipped to interpret the results, while taking into account false negatives and false positives.4
Gene therapy has been successful in mouse models. Adult mice that lack tyrosinase activity have associated retinal functional abnormalities and photoreceptor loss. Intraocular administration of an adeno-associated, virus-based vector encoding the human tyrosine gene has resulted in reversal of the retina anomalies. This may be a preview of very exciting and promising future treatments. For now, we must aim to support our patients and their families with traditional ophthalmologic care and new low-vision devices. REVIEW
Dr. DiMiceli is a pediatric ophthalmology attending at SUNY Downstate Medical Center in Brooklyn, N.Y.
1. Taylor D, Hoyt CS. Pediatric Ophthalmology and Strabismus: Third Edition. Edinburgh: Elsevier- Saunders 2005.
2. Seward Jr S. Hermansky-Pudlak Syndrome: Health Care Throughout Life. Pediatrics 2013;132:153-160.
3. Levin A, Stroh E. Albinism for the Busy Clinician. J AAPOS 2011;15:59-66.
4. Kutzbach B, Merrill K, Hogue K, Downes S. Evaluation of vision specific quality-of-life in albinism. J AAPOS 2009;13:191-195.
5. Hertle R, Yang D, Shatnawi R. Effects of extra-ocular muscle surgery on 15 patients with oculocutane-ous albinism (OCA) and infantile nystagmus syndrome (INS). Am J Ophthalmol 2004:138:978-87.
6. Cronin T, Hertle R, Ishikawa H, Schuman J. Spectral domain optical coherence tomography for detection of foveal morphology in patients with nystagmus. J AAPOS 2009;13(6):563-566.
7. Barot N, McLean R, Gottlob I. The effect of colored overlays on reading performance in infantile nys-tagmus. Ophthalmology 2014;121:804-5.e2. doi: 10.1016/j.ophtha.2013.10.026. Epub 2013 Dec 4.
8. Anderson J, Lavoie J, Merrill, K. Efficacy of spectacles in persons with albinism. J AAPOS 2004;8:515-520
9. Yahalom C, Tzur V, Blumenfeld A, Greifner G. Refractive profile in oculocutaneous albinism and its correlation with final visual outcome. Br J Ophthalmol 2012;96:537-9. doi: 10.1136/bjophthalmol-2011-300072. Epub 2011 Dec 1.
10. Mohammad S, Gottlob I, Kumar A. The functional significance of foveal abnormalities in albinism measured using spectral-domain optical coherence tomography. Ophthalmology 2011;118:1645-52


